Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us
Denied claims are one of the most common frustrations in a medical practice. They are rarely random. Most denials happen because of coding errors, missing documentation, incorrect patient data, or payer-specific rule mismatches. These mistakes delay payment, increase administrative workload, and raise audit risk. Many physicians assume their billing system, or clearinghouse, will catch errors automatically, but weak claim scrubbing allows revenue to leak daily.
Claim scrubbing is a critical control point. When done properly, it prevents rejections and denials, improves cash flow, and reduces compliance exposure. When done poorly, it creates repeat errors, rework costs, and stress during audits. This guide explains how claim scrubbing works, why it matters, and how practices can strengthen it to protect revenue.
Claim scrubbing is the process of reviewing a medical claim before it is submitted to the payer. The goal is to catch errors that would cause rejection or denial. Claims include CPT procedure codes, ICD-10-CM diagnosis codes, HCPCS codes for supplies or drugs, patient and provider identifiers, and sometimes modifiers.
A rejection occurs when a claim is returned immediately due to missing or incorrect information. A denial occurs after the payer processes the claim and determines it will not pay. Claim scrubbing primarily prevents rejections and many front-end denials, helping practices submit clean claims from the start.
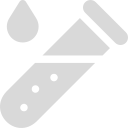
Revenue Cycle Management (RCM) covers the entire financial workflow of a patient encounter, from scheduling to payment. Claim scrubbing occurs after coding but before submission to the payer. A typical sequence is: provider documentation in the EHR, coder assigns CPT and ICD-10-CM codes, billing prepares the claim, claim is scrubbed internally, and then transmitted to a clearinghouse or payer.
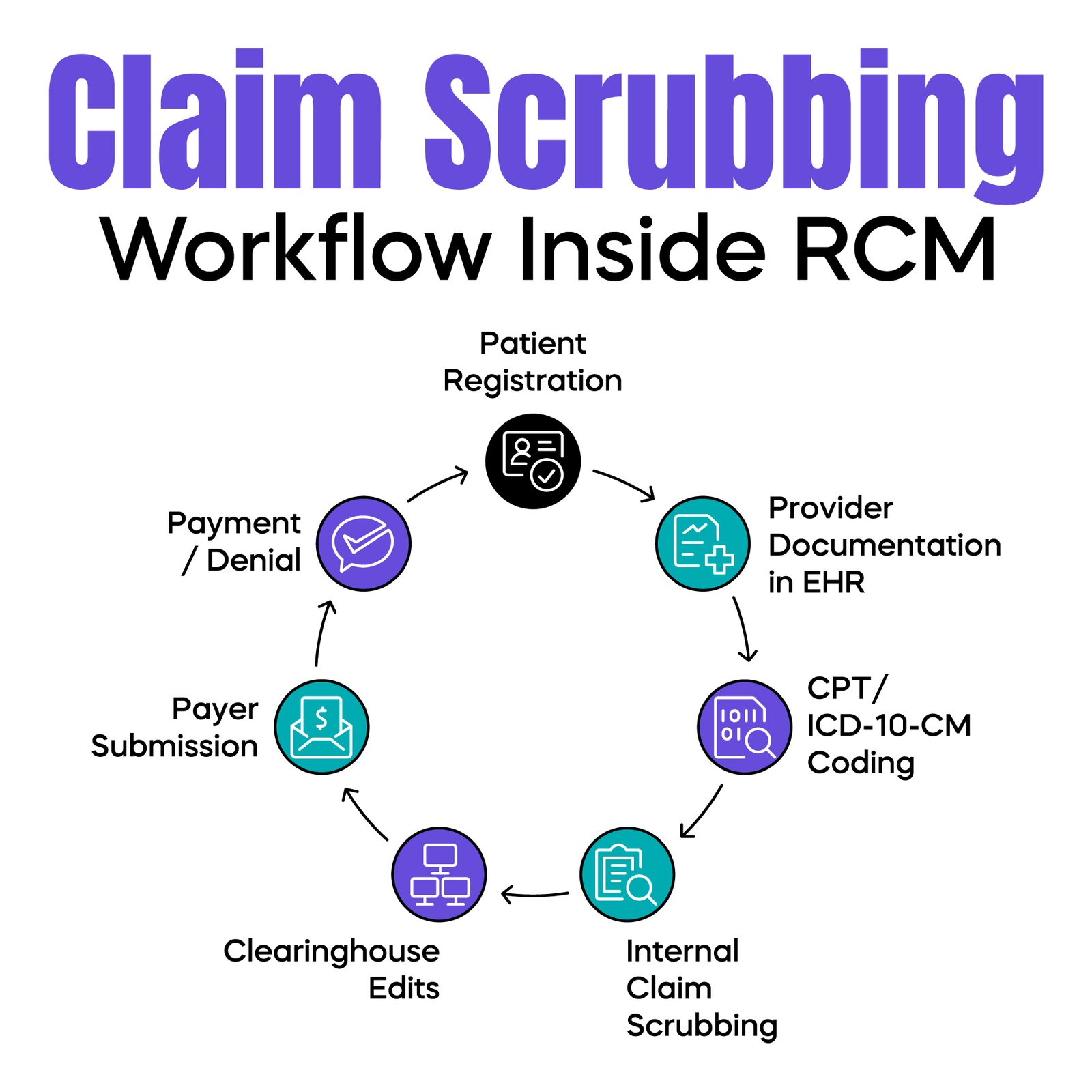
Clearinghouses perform basic edits, but relying solely on them is risky. They mostly check formatting and basic code validity. They rarely apply payer-specific rules, LCDs, or NCDs. Strong claim scrubbing must occur within the practice workflow before the claim leaves the office.
Claim scrubbing combines automated software checks and human review.
First, patient demographics are verified. Incorrect dates of birth, policy numbers, or subscriber information often cause immediate rejections.
Next, coding logic is validated. CPT codes must match ICD-10-CM diagnoses. For example, preventive visit codes billed with problem-focused diagnoses are commonly denied.
Modifiers are checked carefully. Modifier misuse is a top cause of denials. Modifier 25, for instance, requires documentation showing a separately identifiable evaluation and management service on the same day as a procedure. Incorrect use can trigger recoupments in CMS audits.
Frequency limits are reviewed. Some services are allowed only once per year or per lifetime. Prior services must be verified in the EHR before submission.
Finally, payer-specific edits are applied. Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs) define coverage rules. Claims failing these rules may be denied for lack of medical necessity.
Claim scrubbing should identify missing provider identifiers, incorrect place of service codes, mismatched gender-specific procedures, invalid code combinations, and outdated or deleted CPT codes.
Diagnosis sequencing is critical. Many payers require the primary diagnosis to justify the main procedure. Incorrect sequencing can lead to denials even when all codes are otherwise correct.
Prior authorization mismatches must also be flagged. If authorization is required but not documented, the claim may be denied.
A primary care clinic billed minor procedures alongside office visits and automatically appended Modifier 25 to most encounters. Initial payments were approved, but months later, a Medicare audit flagged unsupported Modifier 25 claims. Payments were recouped, and penalties applied.
The root cause was weak scrubbing. The system checked for the modifier’s presence but not documentation support. A strong claim scrubbing workflow would flag high-risk modifier patterns and require verification before submission.
Claim scrubbing is not just about payment speed. It is a compliance safeguard. Improper coding can trigger audits under CMS programs, particularly high-level E/M codes or modifier patterns. Consistent, accurate scrubbing reduces exposure to targeted reviews and recoupments.
High denial rates signal risk to payers. Patterns of repeated errors can trigger audits. Preventive scrubbing is more cost-effective than post-denial corrections.
Clearinghouses act as intermediaries and perform basic edits. They do not fully protect practices from payer-specific policies or documentation gaps.
Internal scrubbing integrates coding edits, payer rules, and documentation checks. The most effective workflow combines both: thorough internal scrubbing followed by clearinghouse validation.
Modern practice management systems include automated rule engines that update CPT and ICD-10-CM codes annually and allow custom rule creation.
Advanced RCM platforms analyze denial trends. They flag repeated payer denials proactively. AI tools can compare EHR documentation with coding selections, reducing undercoding and overcoding risks.
Human oversight is still essential. Technology cannot replace verification of documentation quality and clinical judgment.
Clean claim rate measures claims passing without rejection or denial. First-pass resolution rate tracks claims successfully paid on the first submission. Denial rate by payer highlights high-risk carriers. Days in Accounts Receivable reflect scrubbing efficiency.
Monitoring these metrics allows the practice to identify patterns and adjust scrubbing rules proactively.
Payer policy lag: Practices may update CPT codes annually but miss mid-year LCD changes, causing sudden denial spikes.
Telehealth coding: Temporary or expired codes for remote visits can trigger rejections if systems are not updated promptly.
Coordination of benefits: Incorrect primary-secondary sequencing delays payments. Scrubbing must validate the insurance hierarchy before submission.
Start with accurate patient data capture. Errors at registration often propagate to denials.
Educate coders regularly on CPT updates, ICD-10-CM changes, and payer-specific policies.
Run weekly internal edit reports to identify recurring errors. Adjust system rules as needed.
Integrate documentation audits for high-risk codes such as Modifier 25, Modifier 59, and high-level E/M services.
Maintain clear communication between providers and billing staff to resolve documentation gaps immediately.
Clean claims are paid faster, reduce administrative burden, and improve revenue predictability. Even small reductions in denials can have a significant financial impact, especially for solo or small practices.
Claim scrubbing is essential for reducing denials, protecting revenue, and minimizing compliance exposure. It is both a financial and operational safeguard. Practices that implement structured, proactive scrubbing achieve stronger cash flow, lower administrative burden, and a more audit-ready workflow. Preventing errors before submission is always more effective than correcting them afterward.
Arj Fatima is a U.S. medical billing and RCM specialist with hands-on experience in CPT and ICD-10-CM coding, modifier audits, denial management, CMS compliance, and payer policy interpretation. She helps physician practices reduce denials, strengthen documentation, and implement audit-ready billing workflows.
Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.