Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us



Urologists often lose payment for procedures they clearly performed. The problem is rarely the procedure itself. It is documentation and coding accuracy. CPT code 52007 is a common example.
Many physicians perform ureteral catheterization and collect diagnostic samples, but the operative note does not clearly support the work done. The billing team then selects the wrong code, or the payer downcodes the claim. In some cases, the claim is denied completely.
The biggest confusion comes from mixing simple catheterization with a brush biopsy. These are not the same services. If your documentation does not clearly prove that a brush biopsy was performed, your practice risks losing legitimate reimbursement and increasing audit exposure.
This guide explains CPT code 52007 in clear, simple terms. It focuses on real billing risks, documentation rules, and how to avoid costly mistakes.
CPT code 52007 describes cystourethroscopy with ureteral catheterization and a brush biopsy of the ureter or renal pelvis.
In simple terms, the physician inserts a scope into the bladder, advances a catheter into the ureter, and then uses a small brush to collect cells from the lining of the upper urinary tract.
It is important to understand that this is a cytology procedure, not a traditional tissue biopsy. A brush biopsy collects cells for microscopic evaluation, while a tissue biopsy (such as a forceps biopsy during ureteroscopy) collects actual tissue. This distinction matters because it separates CPT 52007 from ureteroscopy biopsy codes like 52354.
The brush biopsy is the defining element of this code. Without it, the procedure does not qualify for 52007.
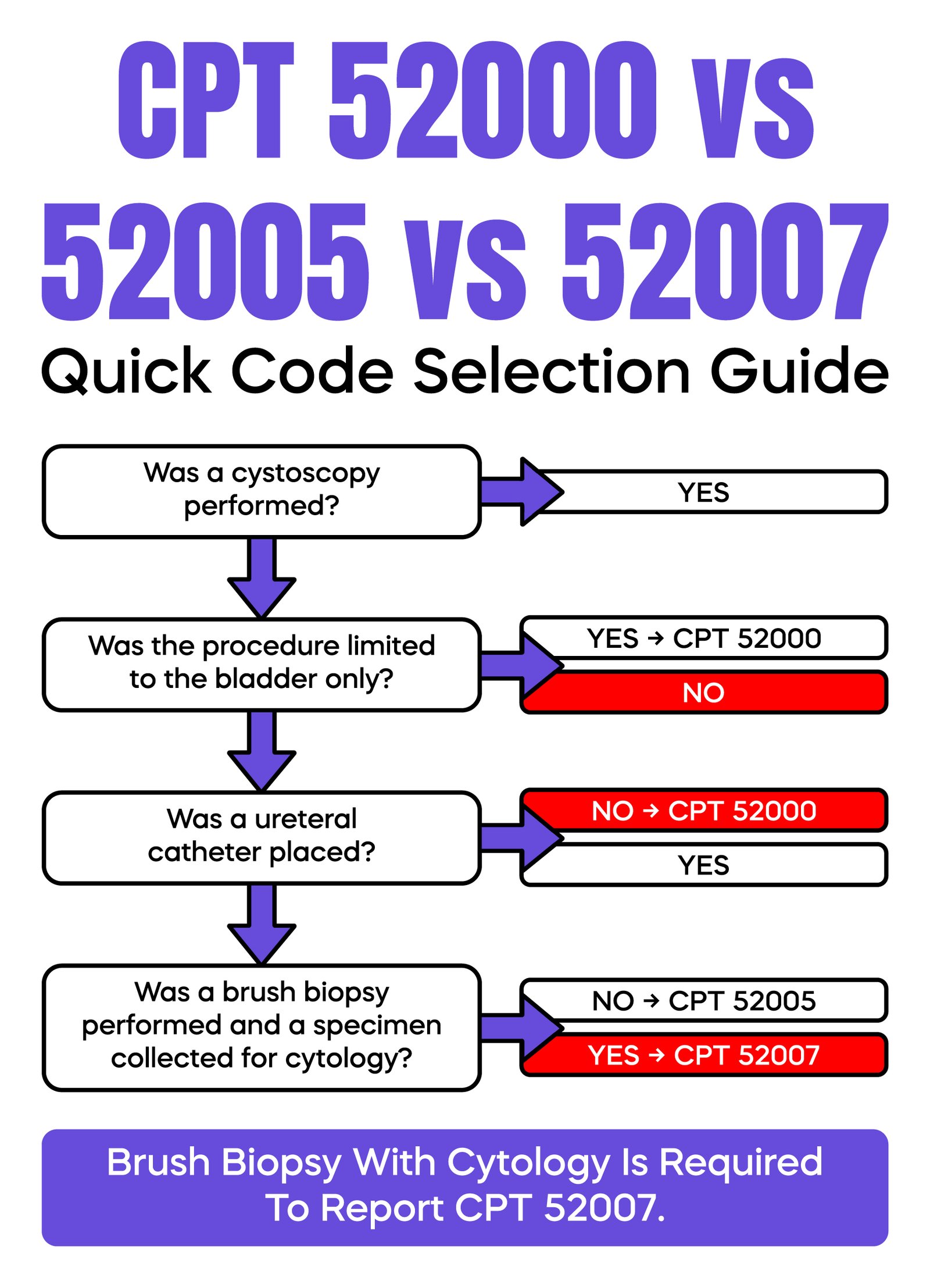
Correct code selection depends entirely on what was performed and documented.
CPT 52000 is used for diagnostic cystoscopy limited to the bladder. CPT 52005 is used when a catheter is passed into the ureter, often for contrast injection or imaging. CPT 52007 includes catheterization but adds a brush biopsy, making it more complex and higher value.
A common real-world mistake occurs when a physician performs catheterization and imaging, but no biopsy. The coder selects 52007 based on an incomplete understanding. The payer reviews the note, finds no biopsy, and either denies the claim or reduces it to 52005.
Another issue arises when documentation is vague. Phrases such as “ureter evaluated” do not support 52007. The payer needs clear proof that a brush biopsy was performed and a specimen was collected.
You should only report CPT 52007 when the catheter is placed, a brush biopsy is performed, and a specimen is obtained for cytologic evaluation. If any of these elements are missing, a different code must be used.
The brush biopsy is not a passive step. It is an active sampling technique that directly impacts reimbursement.
During the procedure, a small brush is advanced through the catheter to the target area. The physician makes multiple passes against the lining of the ureter or renal pelvis to collect cells. These cells are then sent for cytology testing.
Payers expect to see clear documentation of this process. This includes the exact site of sampling and confirmation that a specimen was collected. If the note does not clearly describe this step, the payer may assume no biopsy was performed and deny or downcode the claim.
Documentation determines whether this code is paid or rejected.
The operative report must clearly describe cystoscopy, ureteral catheter placement, use of a brush, the exact site of biopsy, and confirmation that a specimen was collected and sent for cytology. The reason for performing the biopsy must also be stated.
Weak documentation is one of the most common causes of denial. A note that simply states “cystoscopy performed, ureter evaluated” does not support CPT 52007.
A stronger example would clearly state that a catheter was advanced into the ureter, a brush was used at a specific location, multiple passes were made, and a specimen was sent for cytologic analysis.
Another important compliance point is report linkage. If a biopsy is billed, there must be a corresponding cytology or pathology report in the patient record. If this report is missing, the claim may be flagged during audit.
EHR templates are a known risk. Many templates include generic cystoscopy language but do not capture biopsy details. Physicians must update the note manually when a brush biopsy is performed.
Accurate billing requires alignment between documentation, coding, and claim submission.
The procedure is billed using the CMS-1500 form, which is the standard format for submitting professional claims. Before reaching the payer, the claim is reviewed by a clearinghouse to identify errors such as missing diagnosis codes, incorrect code combinations, or incomplete provider information.
A frequent issue is a mismatch between the diagnosis and the procedure. If the diagnosis does not justify a biopsy, the payer may deny the claim for lack of medical necessity.
Revenue cycle performance depends on accuracy at every step. Even small inconsistencies can delay or reduce payment.
Medical necessity must be clearly supported.
The diagnosis code must explain why a brush biopsy was required. General or nonspecific diagnoses often lead to denial. Payers expect to see conditions such as hematuria, suspicious imaging findings, or concern for malignancy.
The diagnosis must create a clear connection between the patient’s condition and the need for cytologic sampling. Without that connection, the claim is at risk.
Modifier use must be precise. Incorrect modifiers are a common source of denials and audits.
Modifier 50 is used when the procedure is performed on both ureters during the same session. Some payers may instead require RT and LT modifiers on separate line items, so payer rules should always be verified.
Modifier 59 may be used only when a distinct and separate service is performed, and documentation clearly supports it. This modifier should be used cautiously, as overuse often triggers payer review.
It is important to note that modifiers 26 and TC do not apply to CPT 52007. This is a surgical procedure code and is not divided into professional and technical components.
In some cases, a retrograde pyelogram is performed during the same session. This imaging service may be billed separately, typically using a radiology code such as 74420.
However, separate billing is only allowed if a full radiologic interpretation is documented. The physician must describe findings such as filling defects or obstruction. Simply mentioning that imaging was used is not sufficient.
Under National Correct Coding Initiative rules, CPT 52007 already includes catheterization and may conflict with other urologic procedures, especially ureteroscopy codes. Improper combinations can lead to automatic denial.
Medicare generally covers CPT 52007 when it is medically necessary. Coverage rules are defined by the Centers for Medicare and Medicaid Services and implemented through regional contractors.
Local Coverage Determinations explain when the procedure is considered appropriate. If documentation does not meet these criteria, the claim may be denied.
Commercial payers often follow Medicare guidelines but may apply stricter requirements, including prior authorization. Practices should always confirm payer-specific policies.
Most denials are preventable and follow predictable patterns.
The most common issue is missing biopsy documentation. The payer reviews the note and finds no clear evidence of a brush biopsy. The claim is then denied or reduced.
Another frequent problem is coding overlap, especially when 52007 is billed alongside ureteroscopy procedures. These combinations are often not allowed.
Denials also occur when there is no cytology report, when diagnosis codes do not support medical necessity, or when bilateral procedures are not properly indicated.
Reducing denials requires consistent documentation, correct code selection, and careful claim review before submission.
| Error | Outcome |
| No brush biopsy documented | Downcoded to 52005 |
| No cytology report | Audit risk or recoupment |
| Vague note (“ureter evaluated”) | Claim denied |
| Wrong diagnosis | Medical necessity denial |
| Incorrect modifier use | Claim rejected |
| Billed with ureteroscopy | NCCI conflict |
CPT 52007 carries a higher audit risk because it involves a biopsy and increased reimbursement.
Payers often monitor how frequently this code is used and whether documentation consistently supports it. Billing a biopsy without corresponding cytology evidence is a major compliance concern.
Practices should conduct internal audits to identify documentation gaps and coding errors early.
Improvement starts with clarity. Physicians must document each step of the procedure in simple, direct language. Coders must confirm that the documentation supports the selected CPT code. Billing teams should review claims for consistency before submission.
Regular training and communication between clinical and billing staff can significantly reduce denials. Small workflow improvements often lead to measurable revenue gains.
CPT code 52007 requires precision. The key element is the brush biopsy and its documentation. If that step is not clearly recorded, the claim will not be paid correctly.
Most denials come from simple issues such as unclear notes, incorrect coding, or missing cytology linkage. These problems are preventable with better documentation and internal review.
Practices that focus on accuracy at every step of the billing process can reduce denials, avoid audits, and protect their revenue.
Arj Fatima is a senior medical billing and coding specialist with hands-on experience in U.S. urology practices. She helps physicians improve CPT accuracy, reduce denials, and stay compliant with federal payer guidelines. Her expertise includes complex coding scenarios, audit defense, and revenue cycle optimization for both solo and multi-specialty practices.


Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

