Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us



OB GYN practices face significant financial and compliance risks when seemingly minor billing errors occur. Revenue loss is rarely due to poor medical care; it is usually caused by compliance gaps that accumulate across multiple claims. Errors such as modifier misuse, billing prenatal visits inside a global package, missing sterilization consent requirements, or mismatched diagnosis codes can trigger denials, recoupments, and audits under the rules of the Centers for Medicare & Medicaid Services. Medicare Administrative Contractors (MACs) rely on data analytics to identify repeated patterns of non-compliance. In real-world reviews, OB GYN practices have experienced six-figure recoupments due to modifier overuse, global maternity billing mistakes, sterilization consent timing errors, and omitted J-codes for devices. Understanding these high-risk areas and implementing structured compliance monitoring is critical for protecting revenue and maintaining regulatory standing.
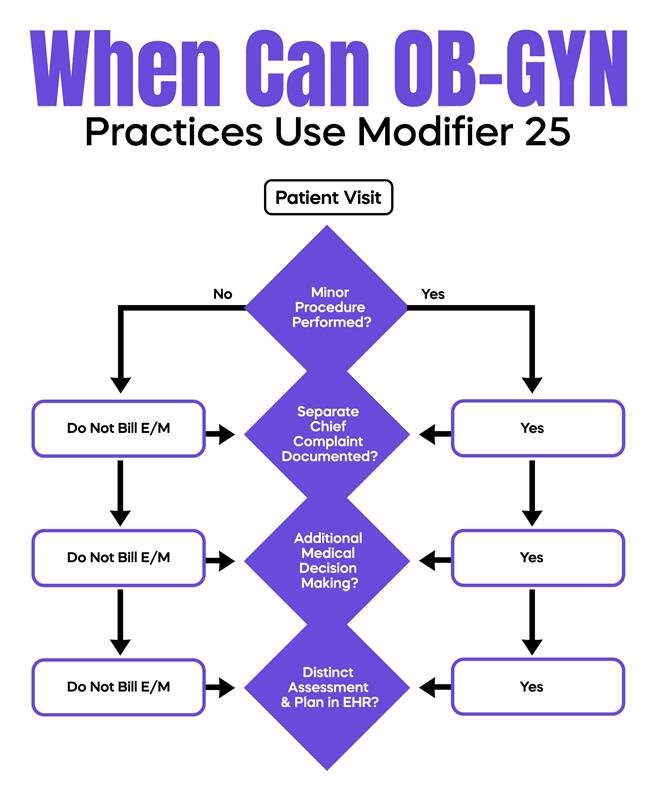
Modifier 25 is frequently audited in OB/GYN practices. It indicates that a significant and separately identifiable E/M service occurred on the same day as a minor procedure. For example, a level 4 E/M visit billed with modifier 25 on the same day as a colposcopy (CPT 57454) requires documentation showing a distinct evaluation. Many denials occur because E/M documentation lacks a separate chief complaint or fails to demonstrate additional medical decision-making beyond the procedural care. MACs compare modifier 25 usage to specialty benchmarks, and practices exceeding expected utilization patterns or X% of procedure encounters may trigger audit review. To reduce risk, documentation should clearly reflect a separate evaluation, individualized assessment, and a distinct medical decision-making process. Structuring EHR notes with separate sections for office visits versus procedures provides visual clarity for reviewers.
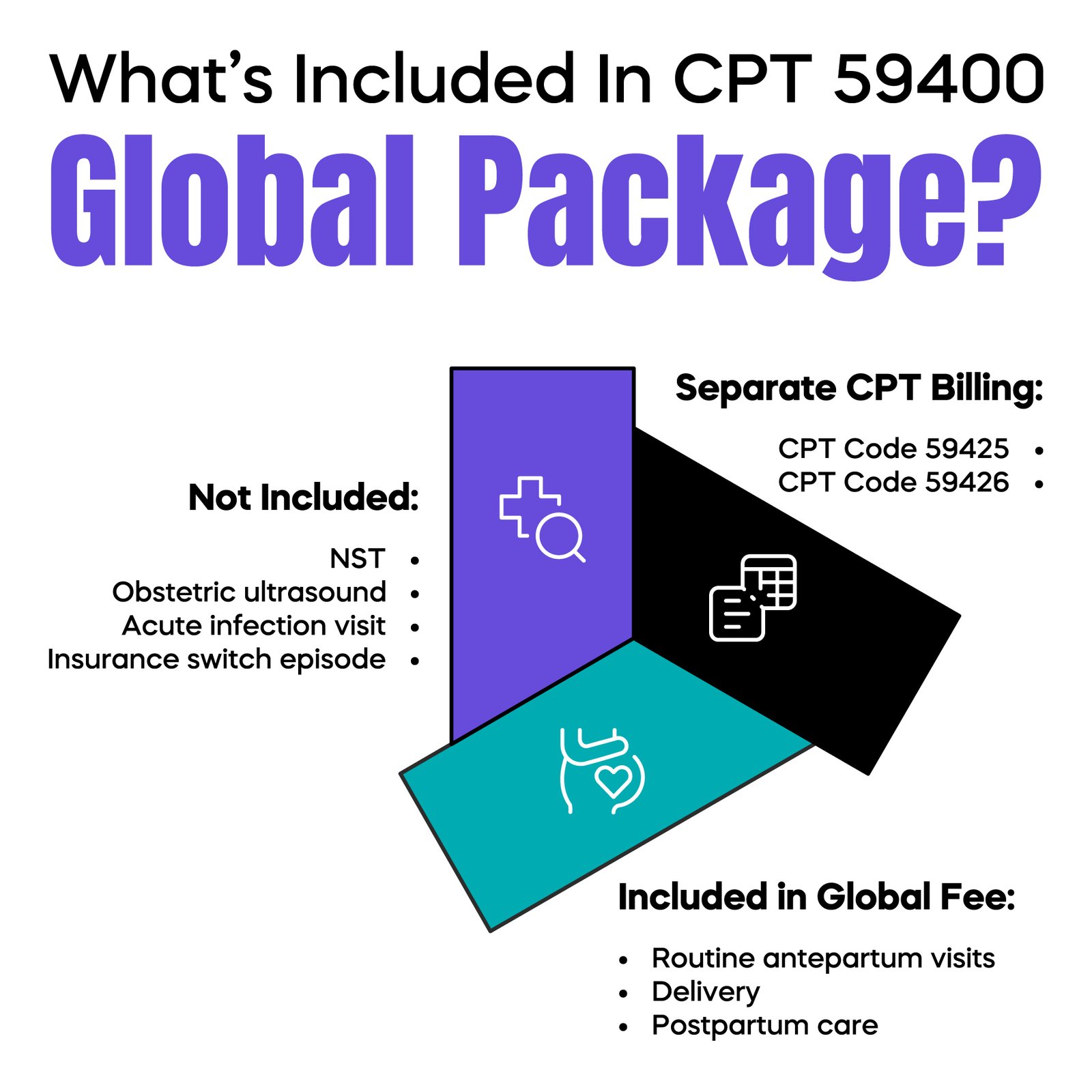
Global maternity packages, such as CPT 59400 and 59510, bundle routine prenatal care, delivery, and postpartum visits into a single payment. While these codes simplify billing, they create frequent compliance traps. Practices often bill routine prenatal visits individually within the global period or fail to unbundle services when a patient switches insurance mid-pregnancy. Antepartum visits should only be billed using CPT 59425 or 59426 when services fall outside the global package, and documentation must support medical necessity. Additional services, including obstetric ultrasounds or non-stress tests, are generally not included in the global fee and require separate billing. Billing unrelated medical issues, such as an acute infection during pregnancy, requires precise documentation demonstrating the encounter is outside routine obstetric care. MACs frequently compare the number of visits per pregnancy episode to specialty benchmarks, and exceeding expected visit counts can trigger audits. Maintaining a pregnancy visit log and reconciling visits against global packages is essential for preventing revenue loss and compliance exposure.
Medicaid sterilization procedures require strict adherence to federal regulations. The HHS-687 consent form must be signed at least 30 full days before surgery, but no more than 180 days prior. Scheduling staff who confirm the existence of a consent form without verifying the signature date risk claim denial for the surgeon, facility, and anesthesia. This single administrative oversight can result in substantial financial loss. Implementing a pre-surgery compliance checklist that confirms the signature date, procedure timing, patient eligibility, and consent validity ensures claims are submitted correctly and reduces audit risk.
Long-Acting Reversible Contraception procedures involve two components: the insertion procedure and the device itself. For example, an IUD insertion (CPT 58300) must be billed separately from the device cost (HCPCS J7298 for hormonal IUD or J7307 for non-hormonal). A common mistake occurs when the physician bills only for the insertion, leaving the high-cost device uncompensated. Additional risk arises during removal and reinsertion on the same day, as some payers require modifiers to prevent automatic bundling. Practices that fail to bill device codes consistently lose significant revenue. Automated billing processes that ensure both procedure and device codes are submitted, along with accurate documentation, mitigate this risk.
E/M services must accurately reflect medical decision-making, either through total time or complexity. Many OB-GYN practices rely on EHR templates, which can produce identical notes across multiple patients. Contractors identify cloned notes by looking for repeated phrasing, identical exam language, and missing individualized assessment. High-level visits billed without supporting documentation for complexity can result in recoupment. Quarterly audits comparing documentation to billed E/M levels, combined with structured template adjustments, ensure compliance and reduce risk.
Gynecologic procedures often carry 0-day or 10-day global periods. Post-procedure visits during these windows related to the same surgical episode are included in the global payment. Billing for routine care during the global period without demonstrating unrelated conditions constitutes overbilling. Conversely, failing to bill legitimate, unrelated visits results in lost revenue. Integrating automated billing alerts to identify active global periods and reconciling claims accordingly prevents both underpayment and overpayment risk.
OB GYN practices frequently perform in-office tests such as pregnancy tests or rapid strep tests. Correct billing requires appending the QW modifier and including a valid CLIA number. Performing tests without current certification violates federal regulations, while omitting the QW modifier can result in denials due to high-volume claim review. Regular CLIA credential audits and proper claim submission processes prevent these avoidable compliance failures.
Incident-to billing allows services provided by mid-level clinicians to be billed under a physician’s NPI only when the physician is physically present and the service follows an established care plan. If a nurse practitioner evaluates a new problem independently, billing under the physician’s NPI violates compliance rules. Place of Service (POS) errors, such as billing POS 11 for procedures performed in an ambulatory surgery center, also create audit risk. Ensuring accurate POS selection and incident-to eligibility verification reduces both financial exposure and regulatory risk.
Accurate ICD-10-CM diagnosis coding is essential. Practices often use screening codes for symptomatic patients, fail to update diagnoses after pathology results, or link unrelated diagnoses to procedures. Claims submitted on CMS-1500 forms must comply with Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs). For instance, submitting a routine screening code where the LCD requires evidence of medical necessity can result in denial. Accurate coding aligned with LCD/NCD guidance ensures compliance and reduces audit exposure.
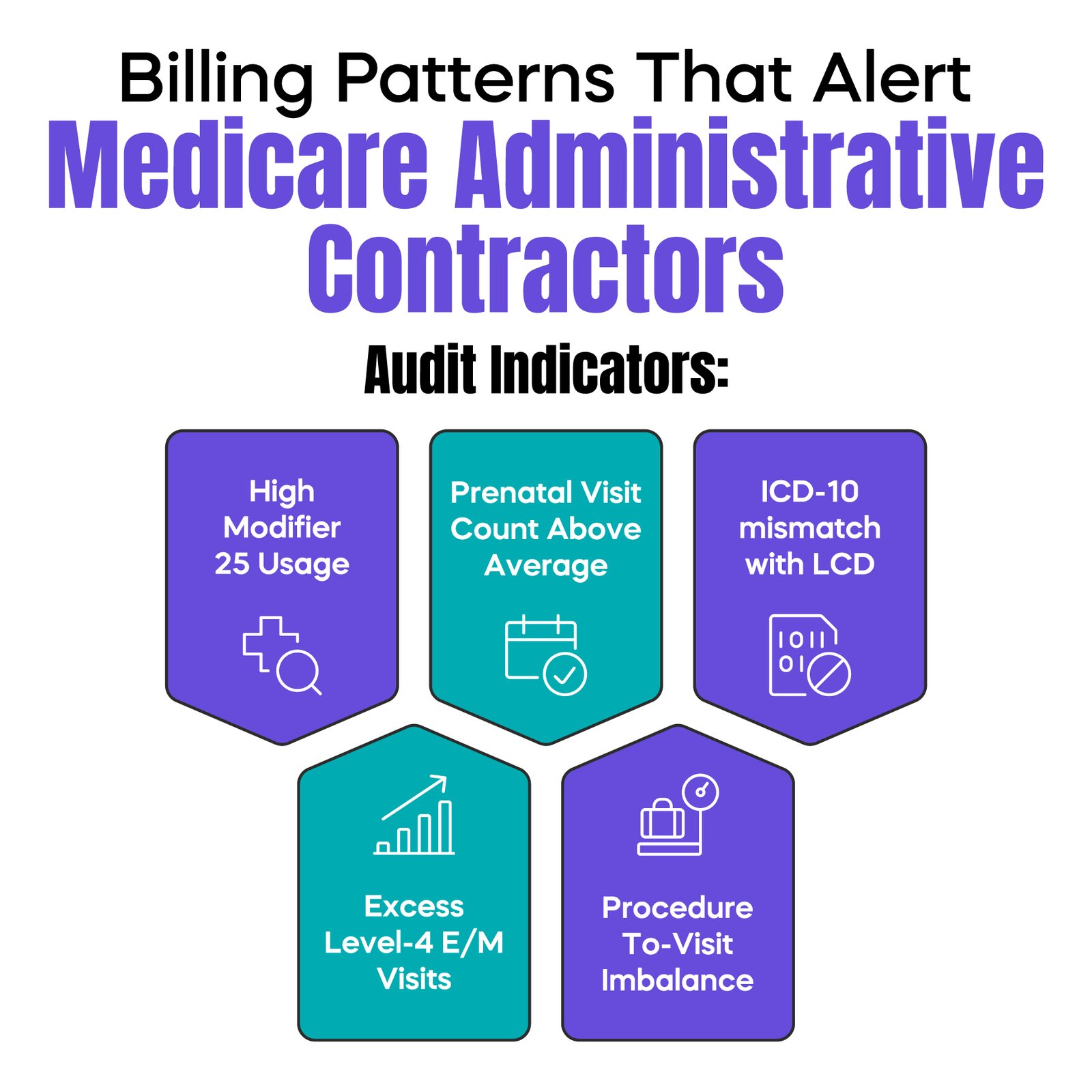
MACs use data-driven analytics to detect billing anomalies. High modifier 25 utilization, frequent high-level E/M visits, unusual procedure-to-visit ratios, and deviations from peer benchmarks all signal potential risk. Practices should monitor these metrics internally, as repeated patterns, rather than isolated errors, typically trigger audits. For example, a practice exceeding X% modifier 25 use in colposcopy encounters may prompt a targeted review. Similarly, submitting more prenatal visits per episode than specialty averages can raise flags.
Preventing billing errors requires structured revenue cycle management. Practices should implement quarterly coding audits, monitor modifier utilization patterns, reconcile pregnancy visits against global packages, verify sterilization consent dates, review J-code billing for devices, monitor global periods, ensure CLIA compliance, and validate incident-to eligibility. Integrating documentation, coding, and operational controls provides a system-level safeguard, reducing both financial and regulatory exposure.
Most gynecology billing compliance mistakes are unintentional, arising from workflow gaps, template cloning, or misunderstanding of payer and Medicare policy. However, repeated errors expose practices to denials, recoupments, and audits. Modifier overuse, global maternity confusion, sterilization timing errors, LARC device omissions, E/M documentation gaps, and incident-to violations are predictable risks. Structured compliance monitoring and integrated revenue cycle management make these errors preventable while protecting physician revenue and regulatory standing.
Arj Fatima is a U.S. medical billing compliance strategist specializing in OB GYN revenue cycle management, CPT coding accuracy, Medicare audit defense, and documentation risk reduction. She helps solo and multi-provider practices identify hidden compliance exposure, correct billing patterns, and implement structured audit-prevention systems that protect physician revenue and regulatory compliance.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

