Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Many physicians lose revenue not because they failed to provide care, but because the service was coded under the wrong category. This problem is common with non-face-to-face services and neonatal care, where coding rules are strict and often misunderstood.
CPT 99445 and CPT 99470 are frequently misused. Some practices confuse them with Remote Patient Monitoring codes, while others avoid using them due to audit concerns. Both situations lead to denied claims, compliance risk, and missed reimbursement.
This guide explains how these codes actually work in medical billing. It focuses on correct usage, documentation, and real-world denial risks so your practice can bill with confidence.
CPT 99445 belongs to the interprofessional consultation code family (99446–99449). These are non-face-to-face evaluation and management services where one physician provides advice to another physician without seeing the patient.
CPT 99470 belongs to the neonatal care services hierarchy. It is used for inpatient care of newborns who require intensive monitoring but do not meet the criteria for critical care.
Understanding these categories is essential. It prevents confusion with unrelated services such as Remote Patient Monitoring or standard E/M visits.
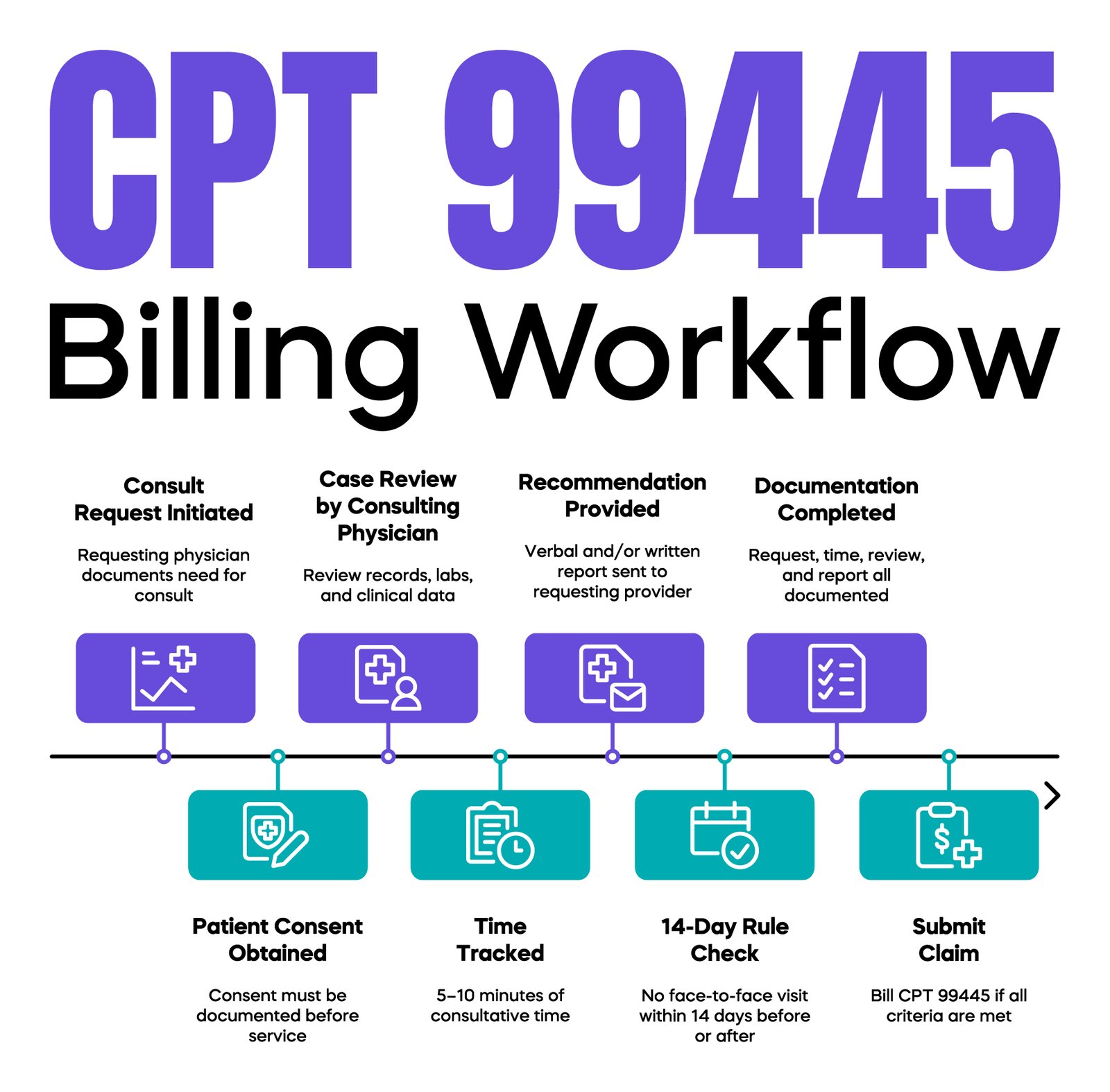
CPT 99445 is used when a physician provides consultative advice to another physician without direct patient interaction.
This code specifically applies to 5 to 10 minutes of medical consultative time.
The consulting physician reviews the patient’s records, evaluates the case, and provides recommendations. A verbal and/or written report back to the requesting provider is required for the service to be complete and billable.
CPT 99445 is part of a structured set of time-based interprofessional consultation codes. CPT 99446 represents 11 to 20 minutes of consultative time, while higher codes such as 99447, 99448, and 99449 apply as total time increases. CPT 99449 specifically requires a written report, unlike other codes in this series that allow verbal communication. This structure allows physicians to select the correct code based on total time spent rather than using a single code for all consultations.
| CPT Code | Time Requirement | Communication Type |
| 99445 | 5–10 minutes | Verbal or Written |
| 99446 | 11–20 minutes | Verbal or Written |
| 99447 | 21–30 minutes | Verbal or Written |
| 99448 | 31+ minutes | Verbal or Written |
| 99449 | 31+ minutes | Written Only |
Select code based on total time and type of report provided.
A practical example involves a primary care physician requesting guidance from a cardiologist for medication adjustment. The cardiologist reviews the case and sends recommendations without seeing the patient. This interaction may qualify for CPT 99445 if all requirements are met.
One of the most important compliance rules is the 14-day restriction.
CPT 99445 cannot be billed if the consulting physician sees the patient:
If a face-to-face visit occurs within this timeframe, the consultation becomes part of the overall evaluation and management service.
This rule is a frequent cause of denials. Many practices document the consultation correctly but overlook the timing requirement.
To support a clean and compliant claim, documentation must be complete and precise.
The requesting physician must document the need for consultation. Patient consent must be obtained and documented before performing interprofessional consultation services. The consulting physician must record the time spent, the clinical review performed, and the recommendations given.
A clear verbal and/or written report back to the requesting provider must be documented, as this is a required component of CPT 99445 and the entire interprofessional consultation code set.
Missing any of these elements can result in claim denial.
A common audit issue occurs when physicians discuss cases informally but fail to document the interaction. In audits, undocumented services are treated as non-billable.
CPT 99470 is used for subsequent inpatient neonatal intensive care, but it does not represent critical care.
It applies to infants who are not critically ill but still require intensive monitoring and physician management.
This level of care is higher than routine newborn care but lower than critical care. The physician is responsible for ongoing evaluation, treatment decisions, and daily documentation.
A typical scenario involves a newborn who is stable but requires close monitoring due to respiratory or metabolic concerns. The physician manages care throughout the day and documents progress, supporting the use of CPT 99470.
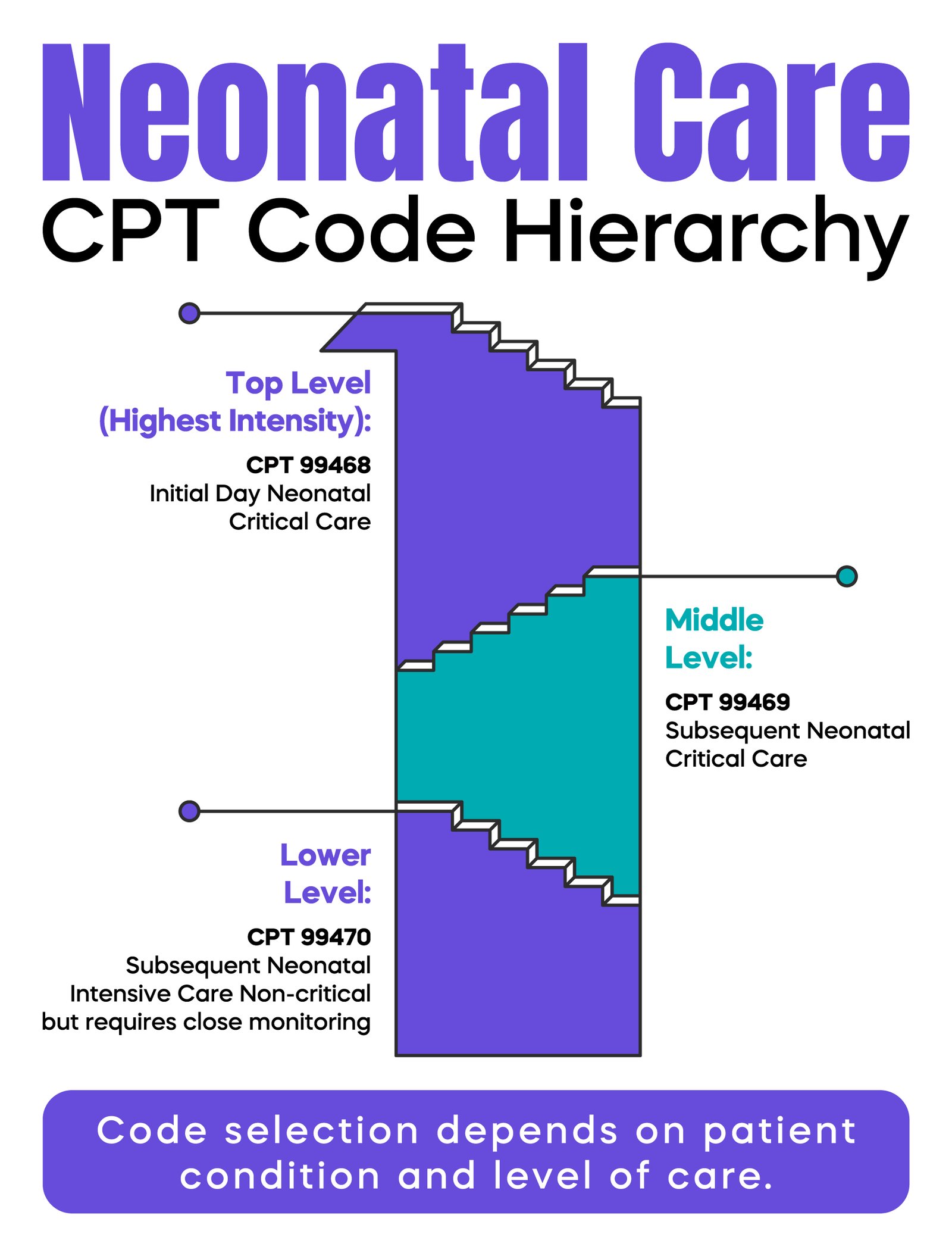
These codes follow a clear hierarchy.
CPT 99468 is used for the initial day of neonatal critical care.
CPT 99469 is used for subsequent days of neonatal critical care.
CPT 99470 is used for subsequent days of neonatal intensive care when the infant is stable but still requires close monitoring.
Misuse of these codes is a common source of audit risk.
Billing CPT 99468 beyond the first day can lead to overbilling. Billing CPT 99470 when the infant meets critical care criteria can result in undercoding or incorrect reporting.
Payers often compare documentation with code selection, making these errors easy to detect.
Denials often follow predictable patterns.
For CPT 99445, the missing documentation of the consultation request is a major issue. Another common problem is billing the code when a face-to-face visit occurs within the 14-day window.
Failure to document the required verbal and/or written report also leads to rejection.
For CPT 99470, lack of medical necessity is a frequent reason for denial. If documentation does not clearly justify intensive monitoring, the claim may be downgraded or denied.
Incorrect placement within the neonatal coding hierarchy is another common issue.
CPT 99445 and CPT 99470 are not part of Remote Patient Monitoring.
RPM codes, such as 99454 and 99457, involve device-based data collection and ongoing patient monitoring.
CPT 99445 is a physician-to-physician consultation service.
CPT 99470 is an inpatient neonatal care service.
Confusing these categories leads to incorrect billing, denials, and compliance risk.
Both codes are frequently reviewed during audits because they depend heavily on documentation.
For CPT 99445, auditors focus on:
For CPT 99470, auditors evaluate:
Repeated or copied documentation in EHR systems can trigger audit concerns.
Accurate billing begins with complete documentation in the EHR.
The coding team assigns CPT and ICD-10-CM codes based on the documented service. Claims are then submitted using the appropriate billing format depending on whether the service is professional or facility-based.
CPT 99470 is typically billed in a hospital setting, and billing workflows may vary depending on how the physician bills relative to the facility.
Errors often occur when documentation does not support the selected CPT code or when diagnosis codes fail to justify the level of care.
Proper coding requires consistent workflows and trained staff.
Billing MedTech helps practices improve documentation accuracy, identify coding errors, and align billing with CMS and payer requirements. This reduces denials and protects revenue without adding administrative burden.
CPT 99445 and CPT 99470 serve very different purposes, but both require a precise understanding to bill correctly. One focuses on physician-to-physician consultation without patient contact, while the other applies to inpatient neonatal intensive care for non-critical infants.
Most revenue loss and audit risk come from simple mistakes. These include missing documentation, incorrect code selection, and misunderstanding of where these codes fit within the broader CPT structure. The 14-day rule, time requirements, and medical necessity standards must be followed closely.
When used correctly, these codes allow physicians to capture legitimate work that is often overlooked. Clear documentation, proper code selection, and awareness of payer expectations are the key factors that protect your claims.
Practices that build strong internal workflows around these requirements reduce denials, improve compliance, and maintain consistent reimbursement.
Arj Fatima is a senior medical billing strategist with over 15 years of experience in U.S. healthcare reimbursement. She specializes in CPT coding, CMS compliance, and revenue cycle management. Arj has helped physicians, solo practices, and specialty groups reduce denials, improve documentation accuracy, and navigate complex payer audits with confidence. Her work focuses on turning complex billing rules into clear, practical workflows for real clinical settings.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

