Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Spine surgeons rarely struggle in the operating room. The real difficulty often begins after the claim is submitted. You complete a technically demanding lumbar fusion. The patient improves. Then weeks later, the explanation of benefits shows a denial. The payer states the decompression was bundled. Or they downcode the case. Or they question medical necessity.
CPT Code 22633 is a high-value lumbar fusion code. It is also heavily reviewed by Medicare and commercial payers. Small documentation gaps can lead to large payment reductions. This guide clarifies how the code works, how reimbursement is calculated, and how to prevent denials under current CMS and payer rules.
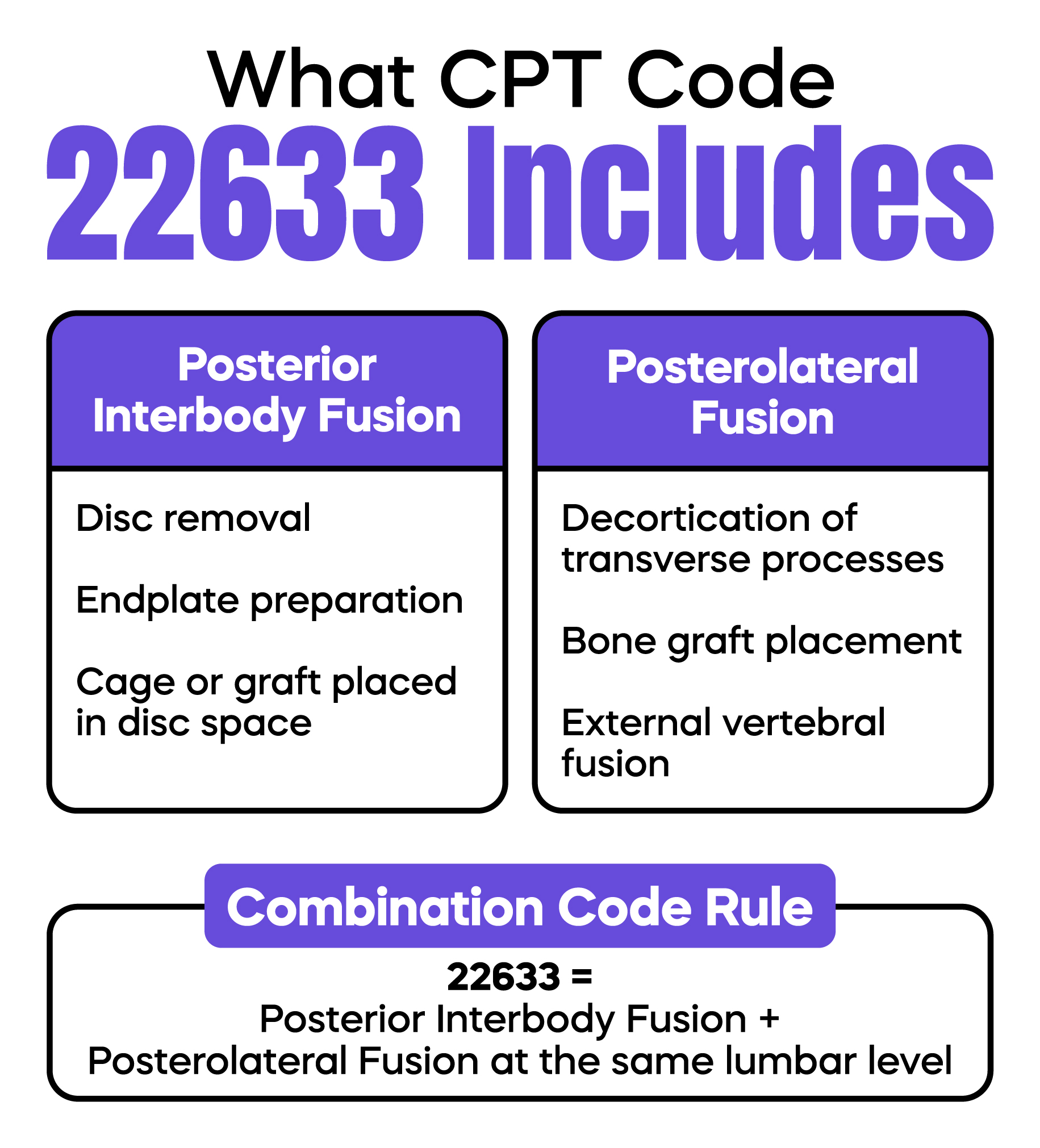
CPT Code 22633 describes a combined lumbar fusion at a single interspace using a posterior approach. It includes both a posterior interbody fusion and a posterolateral fusion at the same level.
An interbody fusion means you remove the disc and place a cage or graft into the disc space. A posterolateral fusion means you place a bone graft along the transverse processes to fuse the vertebrae from the outside.
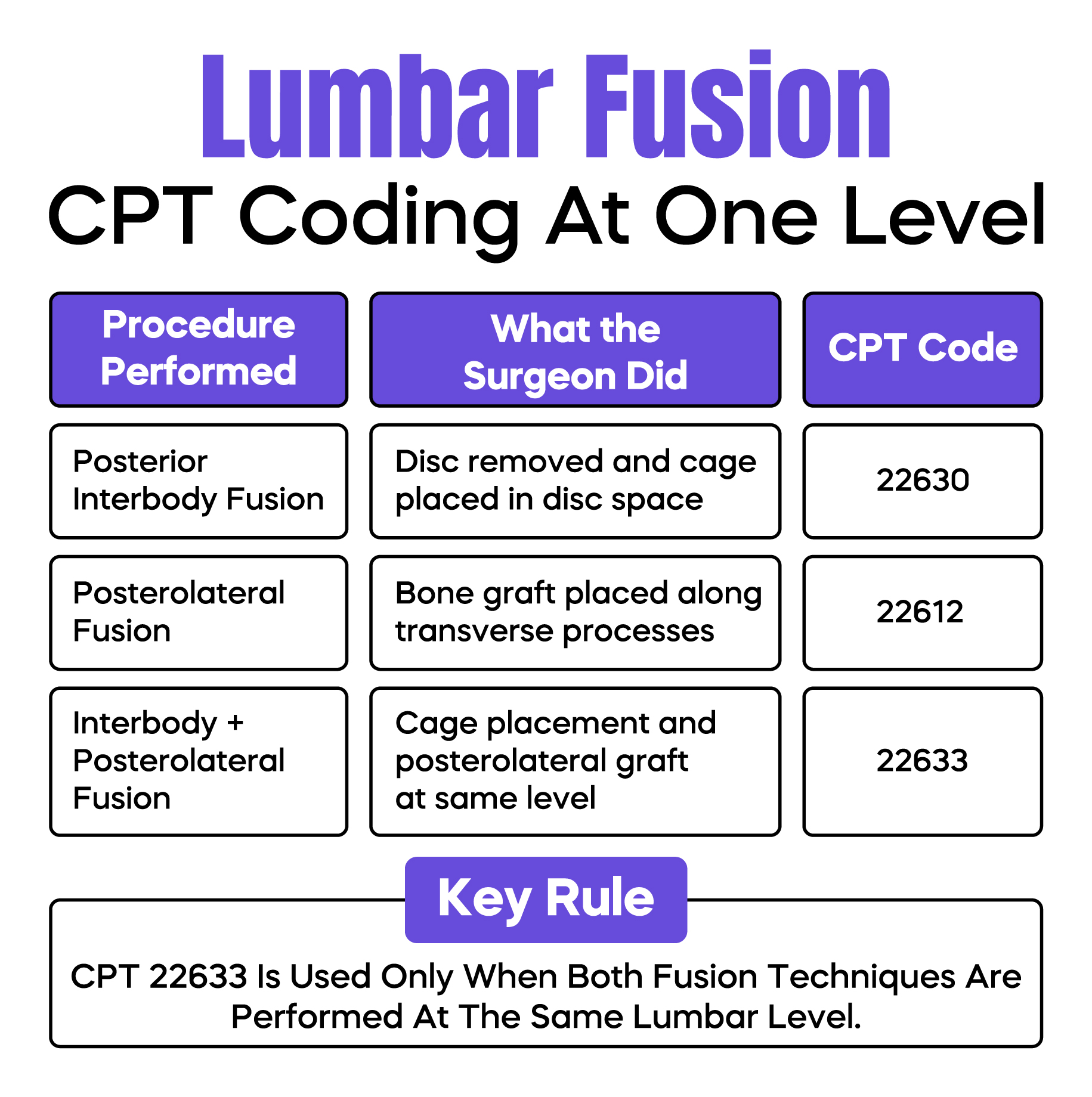
Code 22633 is a combination code created under the Current Procedural Terminology system. It replaced the older practice of billing separate interbody and posterolateral fusion codes at the same level. If you perform both techniques at one lumbar level, 22633 is correct.
If you perform only an interbody fusion, you report 22630. If you perform only a posterolateral fusion, you report 22612. Reporting 22633 when only one technique is performed creates audit risk and potential recoupment.
The most frequent revenue loss occurs when surgeons describe only the cage placement and fail to clearly document the posterolateral graft.
Auditors review three key sections of the operative note:
If the note emphasizes interbody work but does not clearly state that posterolateral fusion was completed, payers may downcode to 22630. That can reduce payment significantly for the same operative effort.
The operative report should clearly state:
Each component must be explicitly documented. Do not assume the reviewer understands what was done.
Medical necessity is defined by the Centers for Medicare & Medicaid Services and interpreted by regional Medicare Administrative Contractors through Local Coverage Determinations.
Most LCDs require documentation of:
Fusion is rarely considered first-line therapy. If preoperative clinic notes do not clearly show failed non-surgical management, payers may deny the claim as not medically necessary.
For example, billing 22633 for isolated lumbar radiculopathy without instability often results in denial. The diagnosis code must support fusion, not just decompression.
Correct ICD-10-CM coding is essential. The diagnosis must reflect the condition treated.
Common supportive diagnoses include lumbar spondylolisthesis, lumbar spinal stenosis with instability, degenerative disc disease with collapse, and recurrent disc herniation with segmental instability.
The diagnosis must match imaging findings and intraoperative documentation. When EHR systems auto-populate vague codes, mismatches occur. These mismatches trigger medical necessity denials.
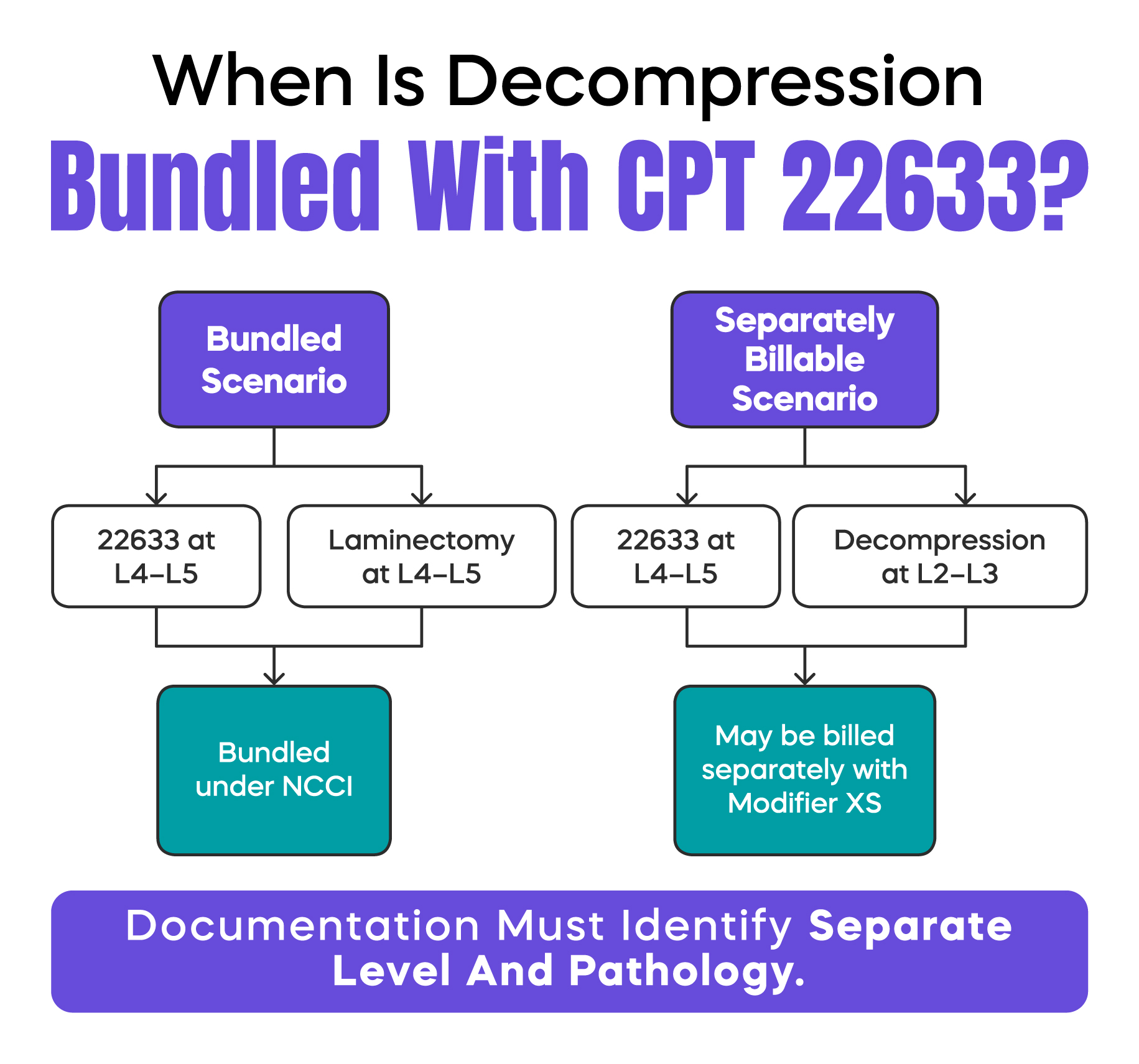
The National Correct Coding Initiative defines which services are bundled together. Under NCCI edits, decompression at the same level as 22633 is usually included.
A common conflict involves decompression code 63047. If you perform a standard laminectomy to access the disc space for fusion, it is considered part of 22633. Billing both codes for the same level will usually result in denial.
However, if you perform a formal decompression at a different level, or if the decompression is clearly separate and more extensive than routine access work, separate reporting may be appropriate with proper modifier use.
The key is documentation clarity. Describe the decompression separately. Identify the level precisely. Explain the pathology treated.
When more than one interspace is fused using the same combined technique, you report 22633 for the first level and 22634 for each additional level.
Code 22634 is an add-on code. It cannot be reported alone. It must follow 22633 on the claim form.
Add-on codes are not subject to multiple procedure payment reductions under the Medicare Physician Fee Schedule. However, incorrect sequencing will cause claim rejection.
Modifier 62 is used when two surgeons from different specialties act as co-surgeons. This is common when an orthopedic spine surgeon and a neurosurgeon collaborate.
However, co-surgery payment is not automatic. Medicare assigns a Co-Surgeon Indicator to each CPT code in the Physician Fee Schedule database. Before billing modifier 62 with 22633, your billing team must verify that the code is eligible under the current Medicare Co-Surgeon Indicator. If the indicator does not allow co-surgery, Medicare will deny the second surgeon’s claim regardless of documentation quality.
When modifier 62 is permitted, both surgeons must perform distinct portions of the procedure and dictate separate operative reports. Each note must clearly describe the specific work completed. Medicare typically increases the allowed amount and then splits the payment between the surgeons. If documentation does not support equal participation, one claim may be denied.
Modifier 59 or the more specific XS modifier may be required when reporting a separate service at a different anatomical level.
For example, if you perform 22633 at L4-L5 and a decompression at L2-L3 for separate stenosis, modifier XS may be appropriate to indicate a separate site.
Improper use of modifier 59 remains a major audit trigger. Always confirm that documentation supports distinct work at a different level.
Modifier 22 may apply if the case required substantially greater effort than typical. Examples include severe scarring from prior surgery, prior instrumentation removal, or complex deformity correction.
The operative report must describe why the work was unusually difficult, how much additional time was required, and what specific factors increased surgical complexity. Without a detailed explanation, payers will ignore the modifier.
Instrumentation is not included in 22633. Posterior fixation must be reported separately using the appropriate instrumentation codes.
Instrumentation selection depends on whether the construct is non-segmental or segmental. Non-segmental fixation, such as fixation across a single interspace without multiple independent anchor points, may be reported with codes such as 22840. Segmental instrumentation involving fixation at multiple vertebral segments may fall under codes 22842 through 22846, depending on the number of segments involved. Accurate code selection requires careful review of the operative construct.
Bone graft codes such as 20930 or 20936 may also be reported when applicable. These are add-on codes and are not subject to multiple procedure reduction when billed appropriately.
CPT 22633 carries a 90-day global period. Routine postoperative care during this period is included in the payment.
Billing an evaluation and management visit within this window requires that the service be unrelated to the fusion. In that case, modifier 24 may be required.
Under the Medicare Physician Fee Schedule, payment for 22633 is calculated using relative value units. These include work RVUs, practice expense RVUs, and malpractice RVUs.
These RVUs are adjusted by geographic practice cost indices and multiplied by the annual conversion factor set by CMS.
Hospital facility reimbursement is separate and typically assigned under the MS-DRG methodology. Ambulatory Surgery Center eligibility depends on CMS and local MAC site-of-service policies.
Most commercial insurers require prior authorization for lumbar fusion. Approval is often diagnosis-specific and level-specific.
If authorization is obtained for decompression only and fusion is added intraoperatively without updated approval, the claim may be denied.
Revenue cycle teams should confirm that authorization details match the final operative report before claim submission.
Spine fusion procedures are high-cost and therefore high audit risk.
Auditors commonly review preoperative conservative therapy records, imaging studies, operative level identification, fusion technique documentation, and instrumentation reporting.
A best practice is a structured pre-bill review for all fusion cases. Coders should confirm that documentation clearly supports both interbody and posterolateral techniques before submission. This step alone can prevent downcoding and post-payment recoupment.
CPT Code 22633 reports a combined posterior interbody and posterolateral lumbar fusion at one interspace. Documentation must clearly support both techniques to avoid downcoding. Decompression at the same level is usually bundled under NCCI rules. Additional levels require add-on code 22634. Co-surgery billing depends on the Medicare Co-Surgeon Indicator. Instrumentation must be coded separately based on whether fixation is segmental or non-segmental. Careful documentation and payer policy review are essential to protect reimbursement and reduce audit risk.
Arj Fatima is a U.S. medical billing and coding specialist with direct experience in spine surgery revenue cycle management. She works with orthopedic and neurosurgical practices to reduce denials, correct modifier misuse, and strengthen documentation for CMS and commercial payer compliance. Her expertise includes CPT validation, ICD-10-CM alignment, NCCI edit analysis, instrumentation coding review, and surgical audit defense strategy.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

