Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Kidney stone Procedures often face delayed payments, not because the surgery was performed incorrectly, but because the claim contained technical errors. For a practice owner, a missing modifier, an unclear operative note, or a mismatch between CPT and ICD-10-CM codes can trigger a denial that stalls cash flow for weeks. CPT code 52356 is a cornerstone of urology stone management, yet it remains one of the most common sources of audit exposure due to bundling and global period misunderstandings.
This guide provides a precise framework for billing 52356. It focuses on documented clinical necessity and National Correct Coding Initiative (NCCI) compliance to help you protect your practice’s revenue.
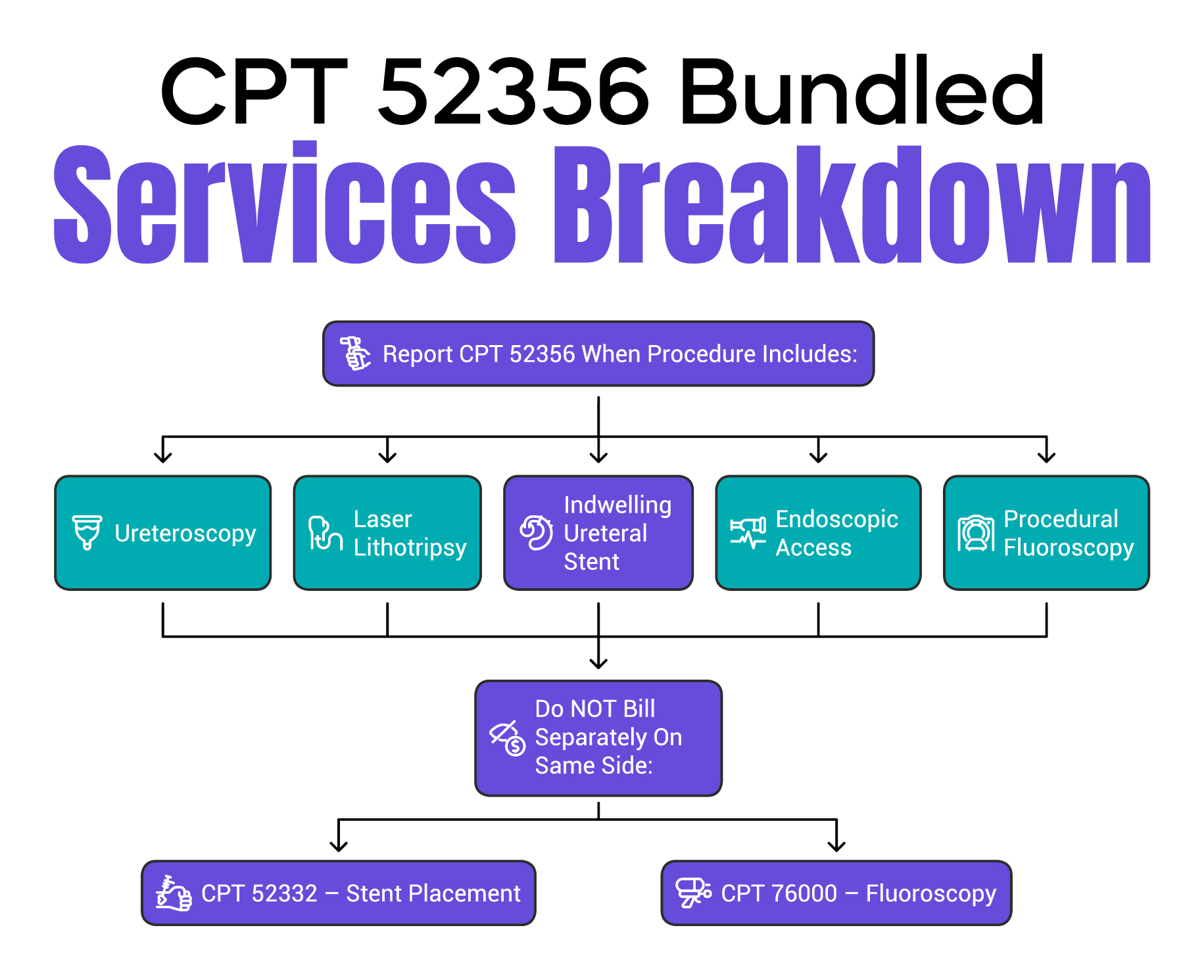
CPT code 52356 describes a comprehensive service: cystourethroscopy with ureteroscopy and/or pyeloscopy with lithotripsy, including the insertion of an indwelling ureteral stent. In plain language, this code covers the doctor inserting a scope through the urethra, accessing the ureter or kidney, breaking the stone into fragments (lithotripsy) using a laser or other energy source, and placing a stent that remains in the patient after discharge.
The most important compliance point is that the stent placement is already bundled into this code. Under NCCI guidelines, you should not bill a separate stent insertion code (such as 52332) when reporting 52356 for the same side of the body. Doing so is considered "unbundling" and will likely trigger an automated payer rejection or a post-payment refund demand.
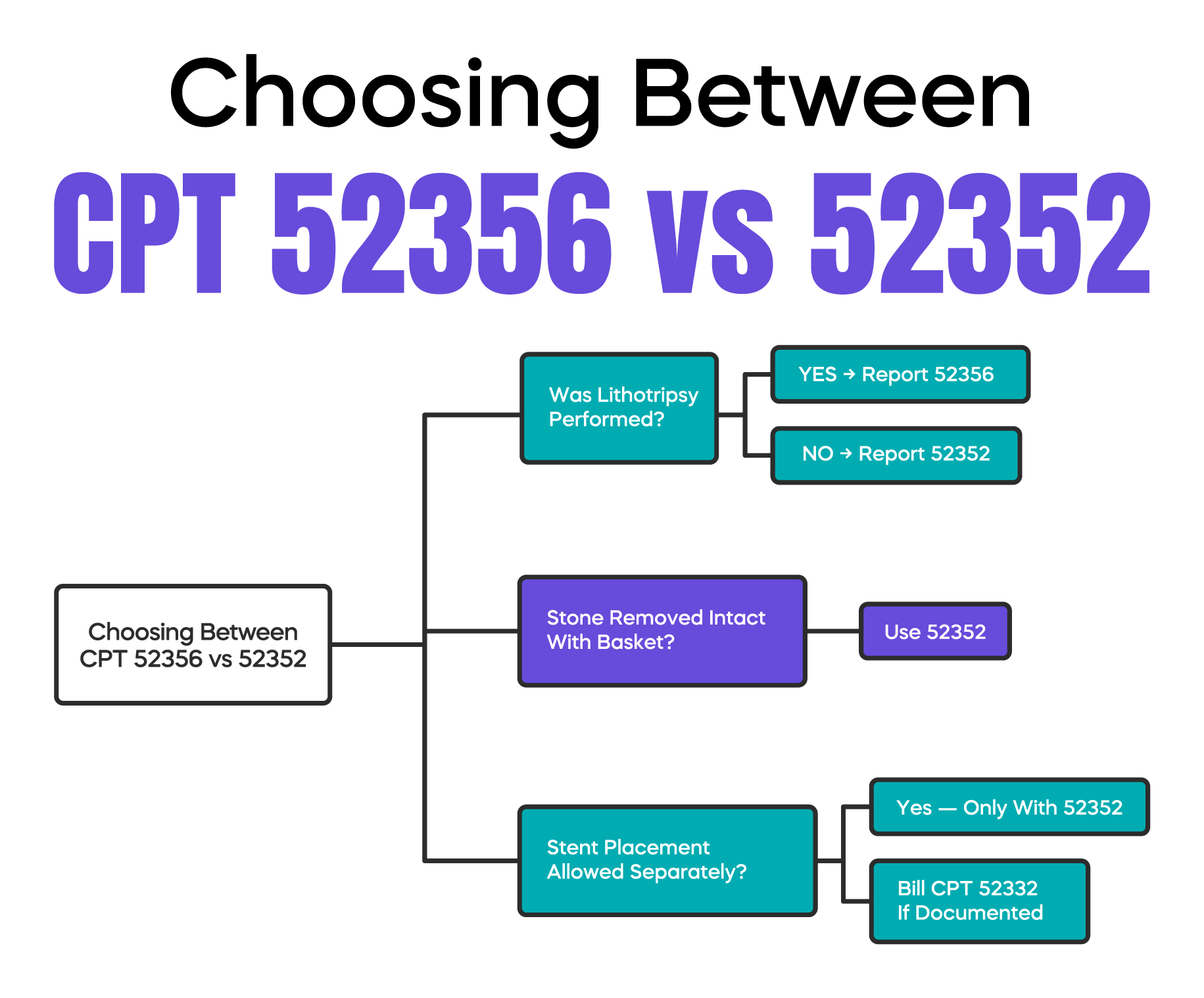
The primary difference between CPT 52356 and other ureteroscopy codes is the method of stone removal and the presence of the stent. You should report 52356 when you fragment a stone (lithotripsy) and leave a double-J or similar stent in place.
If no lithotripsy occurs and the stone is removed intact using a basket, 52356 is not appropriate. In that scenario, you would report 52352 (cystourethroscopy with ureteroscopy and/or pyeloscopy; with removal or manipulation of calculus). Unlike 52356, CPT 52352 does not include the stent, meaning you can often bill 52332 (stent placement) separately on the same side if documented. Always ensure your operative note explicitly uses the term "fragmentation" or "lithotripsy" to justify the use of 52356.
Knowing which services are bundled prevents costly billing errors. CPT code 52356 includes endoscopic access, stone fragmentation, stent insertion, and any fluoroscopic guidance (such as 76000) that is integral to the procedure. Because these are built into the value of 52356, reporting them separately is a major compliance risk.
If you treat multiple stones on the same side (ipsilateral) of the body, for example, one in the ureter and one in the renal pelvis, you still only bill 52356 once. The code covers all stone work on that side. Separate billing is only supported in rare anatomical cases, such as a duplicated collecting system, and requires a modifier like XS (Separate Structure) or 59, supported by an exceptionally detailed operative report.
When treating stones on both the left and right sides during the same session, billing requirements diverge. While commercial payers often accept Modifier 50 (Bilateral Procedure), Medicare Administrative Contractors (MACs) typically prefer you to list the procedure on two separate lines:
Using the incorrect format for your specific payer is a leading cause of "duplicate claim" denials.
It is a common misconception that all endoscopic procedures have a short global window. However, under Medicare and most major payers, CPT 52356 carries a 90-day global period. This means it is classified as a major surgery.
Because of this 90-day window, all routine post-operative Evaluation and Management (E/M) visits are bundled into the surgical fee. You cannot bill separately for follow-up visits related to the recovery from the stone procedure. If a patient returns for an entirely unrelated issue within that 90-day window, you must append Modifier 24 (Unrelated E/M during a global period) to the office visit code to secure payment and avoid an audit flag.
| Billing Component | Rule for CPT 52356 |
| Global Period Duration | 90 Days |
| Modifier for Unrelated E/M | Modifier 24 |
| Modifier for Related Procedure | Modifier 58, 78, or 79 (depending on clinical intent) |
| Included Services | Pre-operative (1 day), Intra-operative, and Routine Post-operative care |
| Audit Sensitivity | High; documentation must clearly differentiate unrelated visits |
When it is time to remove the stent in the office, selecting the correct code is vital. While some practices mistakenly use 52000 (Diagnostic Cystoscopy), the specific code for stent removal is 52310 (Cystourethroscopy with removal of foreign body, calculus, or ureteral stent from urethra or bladder; simple). If the removal is significantly complicated by encrustation or other factors, 52315 may be used, though this requires clear documentation of the complexity.
We recommend that urologists maintain a "Stent Log" to track every insertion and removal date. This ensures patient safety and provides an indisputable trail of medical necessity for your initial 52356 claim.
Strong documentation is the only way to protect your revenue. Your operative report must clearly state:
CPT Code 52356 covers ureteroscopy with lithotripsy and the placement of an indwelling ureteral stent. It is a major surgical procedure with a 90-day global period. Stent placement is bundled and should not be billed separately on the same side. For Medicare billing, use RT and LT modifiers for bilateral cases to ensure clean claim submission.
Arj Fatima is a senior medical billing strategist with over 10 years of experience in U.S. urology revenue cycle management. She specializes in NCCI compliance and complex surgical coding, helping practices maximize reimbursement while minimizing audit risk.


Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.