Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Laceration repair is routine in many practices, but coding errors in these procedures quietly reduce revenue. Many physicians perform the work correctly but lose payment due to small documentation gaps, incorrect code selection, or misuse of modifiers. CPT 12018 is a common example where mistakes happen, especially when wound size, location, or repair type is not clearly documented.
When a patient presents with a facial or mucosal laceration, your clinical focus is on proper repair and cosmetic outcome. However, from a billing perspective, the details you document determine whether you are paid correctly or face denials or audit risk. This guide explains CPT 12018 in a clear, practical way so you can protect revenue without adding complexity to your workflow.
CPT 12018 is used for the simple repair of superficial wounds measuring 7.6 cm to 12.5 cm.
A simple repair means:
The wound involves only the epidermis or dermis
Closure is done using a single layer
No deep tissue repair is performed
This code applies to the following anatomical areas:
This point is often misunderstood. If the same wound length occurs on the arm, leg, or trunk, CPT 12018 does not apply. A different code must be selected.
A common issue occurs when coders select this code based only on wound length while ignoring location. This leads to claim rejection.
Wound repair coding depends on three factors:
All three must match for CPT 12018.
If multiple simple wounds are in the same anatomical group:
Example:
If wounds are in different anatomical groups, report them separately with appropriate modifiers when needed.
CPT 12018 represents a bundled service. It includes local anesthesia, wound cleaning, irrigation, and simple debridement as part of the procedure. Closure using sutures, staples, or tissue adhesives is also included.
Because of this bundling, separate billing for lidocaine injection or basic wound preparation will result in denials. This is a common issue seen in practices that do not follow bundling rules closely.
The closure method also requires attention. Sutures, staples, and tissue adhesives such as Dermabond all qualify under simple repair. However, if only adhesive strips like Steri-Strips are used, the service may not qualify as a repair procedure. In most cases, it is either included in an evaluation and management service or is not separately billable.
Accurate documentation is the primary factor that determines payment.
To support CPT 12018, the medical record must clearly state the exact wound length in centimeters, the precise anatomical location, the type of repair, and the method of closure. The condition of the wound should also be described to support medical necessity.
Vague descriptions such as “large laceration” are not acceptable. A common denial scenario occurs when a provider documents “facial laceration repaired” without recording the length. In such cases, the coder may assign CPT 12018, but the payer will often deny or downcode the claim due to missing information.
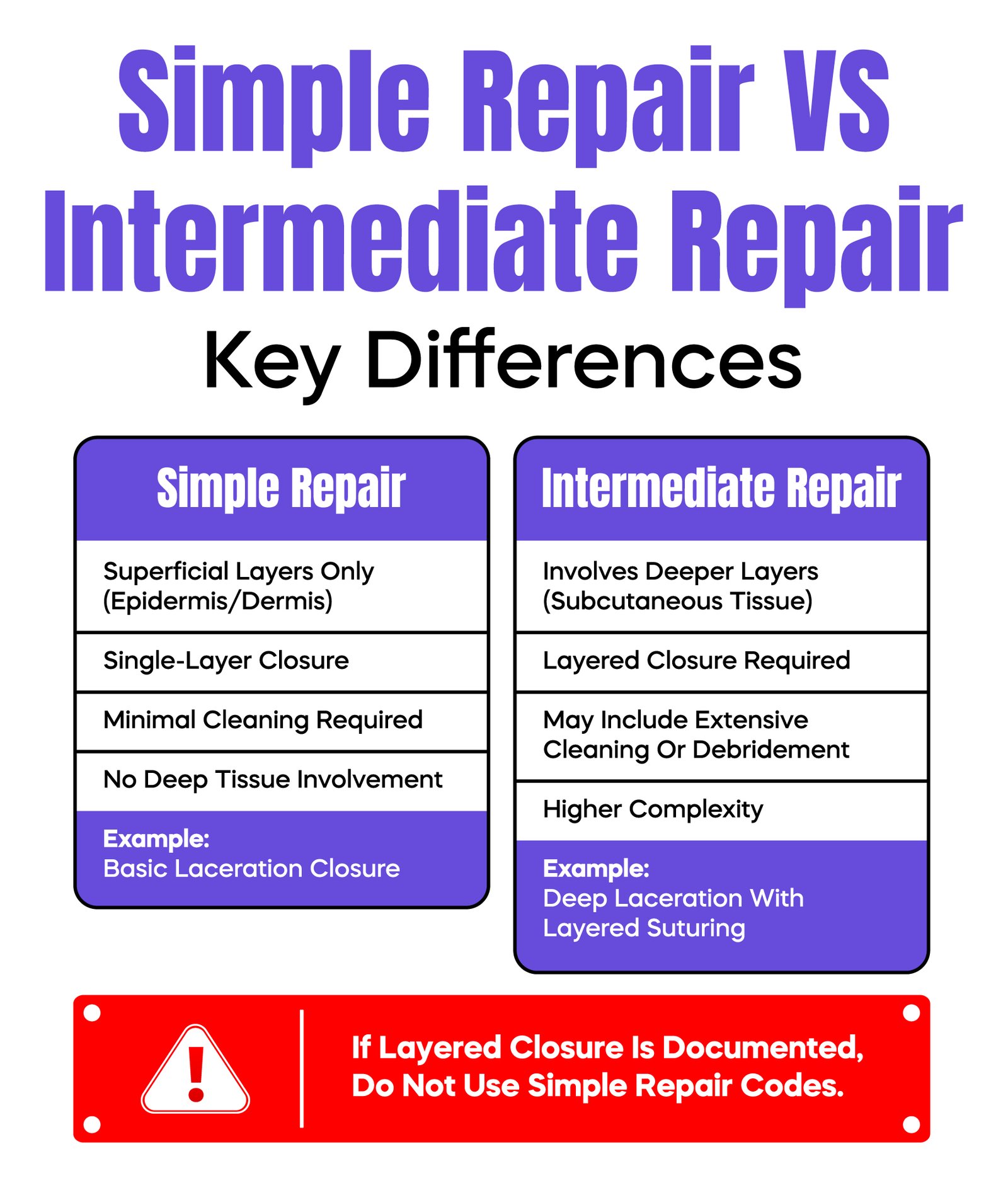
Certain documentation terms also carry risk. Words like “layered closure” or “undermining performed” indicate a more complex repair. If these are documented, the procedure is no longer considered simple, and CPT 12018 becomes incorrect. This mismatch can trigger audits.
Even a small difference in measurement can change the code selection. A wound measuring 7.5 cm falls under CPT 12017, while a wound measuring 7.6 cm qualifies for CPT 12018. This makes precise measurement essential.
Complexity must also be evaluated carefully. If the repair involves deeper tissue layers or requires additional work beyond simple closure, it may qualify as an intermediate repair. In such cases, using CPT 12018 would be incorrect and may lead to undercoding or compliance risk.
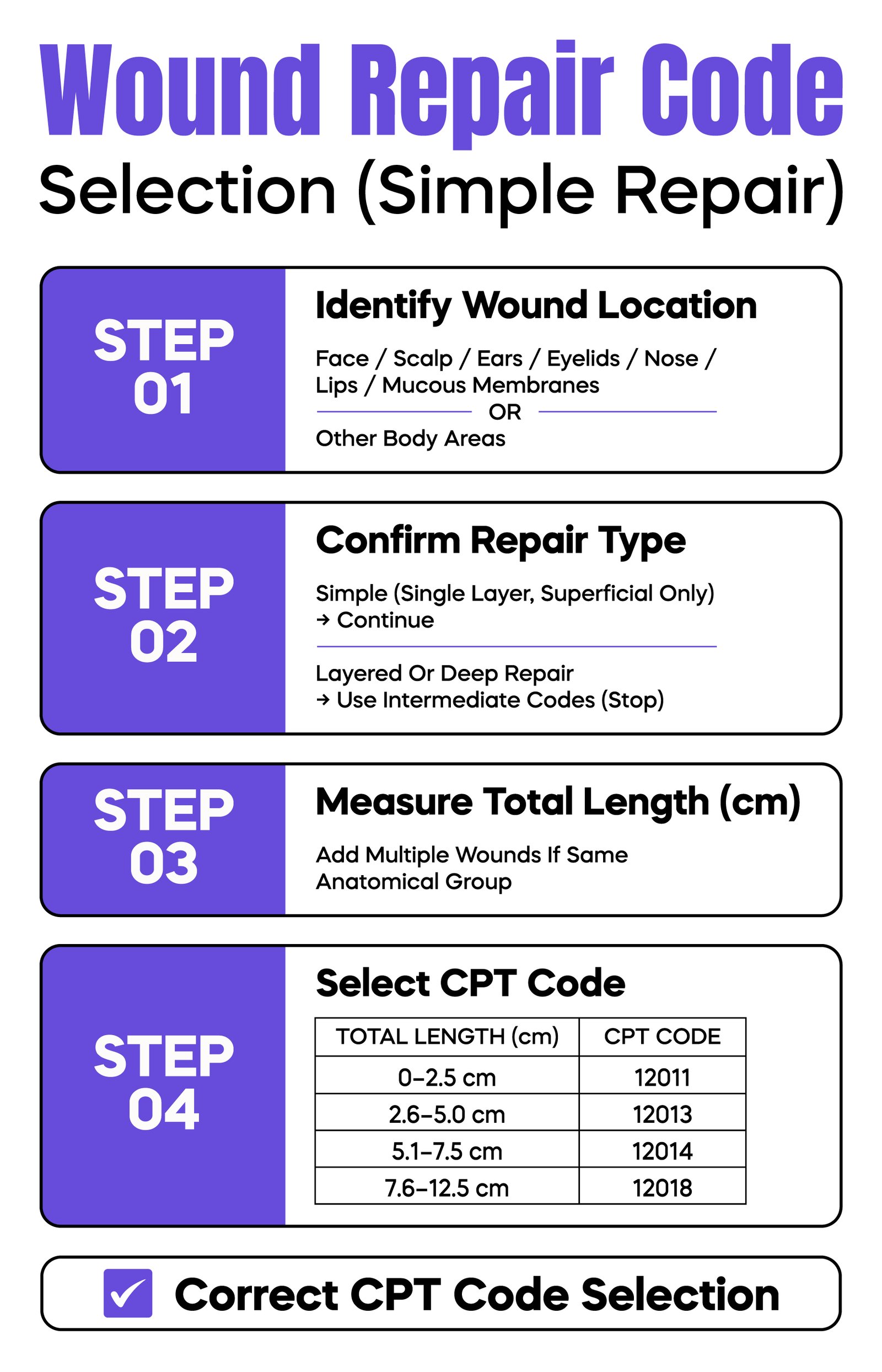
| Wound Length (cm) | CPT Code |
| 0 – 2.5 cm | 12011 |
| 2.6 – 5.0 cm | 12013 |
| 5.1 – 7.5 cm | 12014 |
| 7.6 – 12.5 cm | 12018 |
A structured workflow helps reduce errors and improve claim acceptance.
The process begins with clear documentation in the EHR. The provider must include all required elements such as wound length, location, and repair type. The coder then verifies that the code selection matches these details.
The diagnosis is assigned using ICD-10-CM, and the claim is prepared using CMS-1500. The claim is then submitted through a clearinghouse for validation before reaching the payer.
Any missing or inconsistent information at earlier stages increases the likelihood of denial.
Payment for CPT 12018 varies based on multiple factors. These include the Medicare Physician Fee Schedule, geographic adjustments, the setting in which the service is performed, and payer-specific contracts.
Medicare calculates reimbursement using relative value units, while private payers may follow different methodologies. Underpayment often occurs when documentation is incomplete or when coding is questioned during payer review.
CPT 12018 carries a 10-day global period. This means routine follow-up visits, suture removal, and basic wound checks are included in the original payment and cannot be billed separately.
If a patient returns during this period for a completely unrelated issue, an evaluation and management service may be billed. However, the documentation must clearly support that the visit is separate from the original procedure.
Modifiers must be used with precision because they are closely monitored by payers.
Modifier 25 is appropriate only when a separate and significant evaluation and management service is performed on the same day as the procedure. Overuse of this modifier without proper documentation is a common audit trigger.
Modifier 51 applies to multiple procedures, although some payers handle this automatically. Modifier 59 is used to indicate a distinct procedural service and must be supported by clear documentation showing that the services are not related.
Incorrect use of modifiers is one of the most common reasons for claim rejection.
CPT 12018 is part of a code range that varies primarily by wound length and location. Smaller wounds fall under CPT 12011 or CPT 12017, while CPT 12018 applies to larger wounds within the defined range of 7.6 cm to 12.5 cm.
Another frequent point of confusion is the distinction between simple and intermediate repair. If layered closure is performed, the repair is no longer simple, and CPT 12018 should not be used.
Most denials follow predictable patterns. Missing wound length, incorrect anatomical coding, wrong repair classification, bundling errors, and unsupported modifier use are the most common issues.
For example, some practices routinely attach Modifier 25 to every visit. Payers quickly identify this pattern, which often leads to denials when documentation does not support a separate evaluation service.
Preventing these issues requires consistent provider training, regular coding audits, and ongoing review of denial trends.
Wound repair coding is frequently reviewed during audits. Auditors focus on whether documentation supports the code billed, whether modifiers are used appropriately, and whether the repair type is correctly classified.
Another risk occurs when practices bill a repair code for services that only involve adhesive strips. In such cases, the service does not meet the criteria for a repair procedure.
Repeated inconsistencies between documentation and coding may lead to recoupment of payments. Regular internal audits help reduce this risk.
Improving documentation accuracy has a direct impact on revenue. Providers should document clearly at the time of service, and coders should verify all elements before claim submission.
Denial reports should be reviewed regularly to identify patterns. Even small improvements in documentation and coding accuracy can lead to significant financial gains over time.
Accurate use of CPT 12018 depends on disciplined documentation and correct interpretation of coding rules. The code is straightforward in definition, but small errors in wound measurement, anatomical selection, or repair classification can quickly lead to denials, underpayment, or audit exposure.
In most cases, revenue loss does not occur because the procedure was performed incorrectly. It happens because the documentation does not clearly support the service billed. Missing wound length, incorrect use of modifiers, or misclassification between simple and intermediate repair are the most common failure points.
Practices that maintain consistent documentation habits, verify coding before submission, and monitor denial trends are better positioned to capture full reimbursement while staying compliant. Over time, even minor improvements in these areas can produce measurable financial impact and reduce administrative burden.
Arj Fatima is a senior medical billing and coding specialist with deep experience in U.S. healthcare systems. She works with physicians to improve coding accuracy, reduce denials, and ensure compliance with payer and CMS guidelines. Her expertise includes CPT audits, documentation improvement, and revenue cycle optimization.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

