Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Physicians often treat minor lacerations every day, yet many practices still lose revenue or face denials on these simple cases. The issue is rarely the procedure itself. It is how the repair is documented, measured, and coded. CPT 12001 looks straightforward, but small mistakes can lead to underbilling, payer rejections, or audit exposure. If wound size is not measured correctly, if multiple lacerations are not combined properly, or if the repair type is misunderstood, the claim will not reflect the true work performed. This guide practically explains CPT 12001, using real billing scenarios to help you code accurately and stay compliant.
CPT 12001 is used for simple repair of superficial wounds that are 2.5 centimeters (cm) or less in length. A simple repair means the wound involves only the skin layers, such as the epidermis or dermis. It does not involve deeper tissue like muscle or fascia.
This code applies to the scalp, neck, trunk, extremities, axillae, and external genitalia. It does not apply to the face, eyelids, lips, or ears, which fall under a separate code range.
A simple repair involves a single-layer closure using sutures, staples, or tissue adhesive. Local anesthesia, basic cleaning, and minor debridement are included and cannot be billed separately.
Wound size determines whether CPT 12001 can be used. The total wound length must be 2.5 cm or less.
Accurate measurement must be documented clearly. Vague descriptions like “small laceration” are not acceptable.
If multiple wounds are treated in the same anatomical group and share the same complexity, their lengths must be added together. This is required under CPT coding rules.
For example, three lacerations of 1 cm each on the scalp must be combined to 3 cm. This exceeds the CPT 12001 limit, so CPT 12002 should be billed instead.
Wounds in different anatomical groups cannot be combined.
Failure to follow this rule often leads to underbilling or duplicate claim denials.
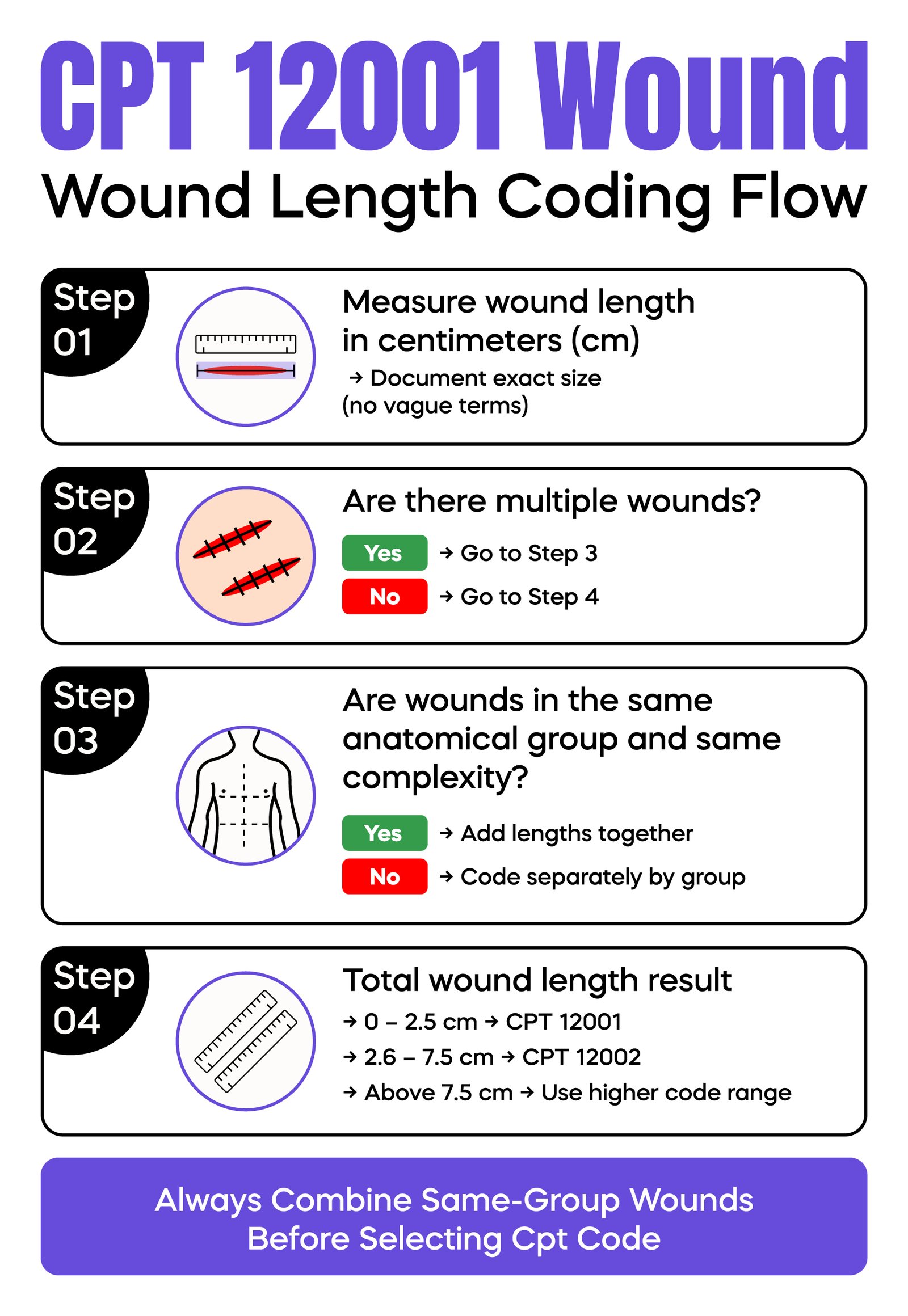
The difference between CPT 12001 and CPT 12002 is based on total wound length.
CPT 12001 applies up to 2.5 cm.
CPT 12002 applies from 2.6 cm to 7.5 cm.
A common real-world issue occurs when providers do not document measurements. Billing teams then default to the lowest code, leading to revenue loss.
Another scenario involves incorrect multiple billing. Two 1.5 cm wounds on the same arm must be combined into 3 cm and billed as CPT 12002, not CPT 12001 twice.
Clear measurement at the point of care prevents both undercoding and compliance risk.
Documentation must fully support the code billed. The provider must record the exact wound length in cm and the precise anatomical location.
The repair type must be clearly stated as simple. The method of closure should be documented, including sutures, staples, or adhesive.
Local anesthesia should be documented even though it is included in the procedure.
Cleaning level matters. Routine irrigation is considered part of a simple repair and does not change the code. However, if the wound is heavily contaminated and requires significant debridement or removal of foreign material, this may qualify as an intermediate repair. This must be clearly documented.
A frequent denial occurs when the wound size is missing. Without this, the payer cannot validate the claim.
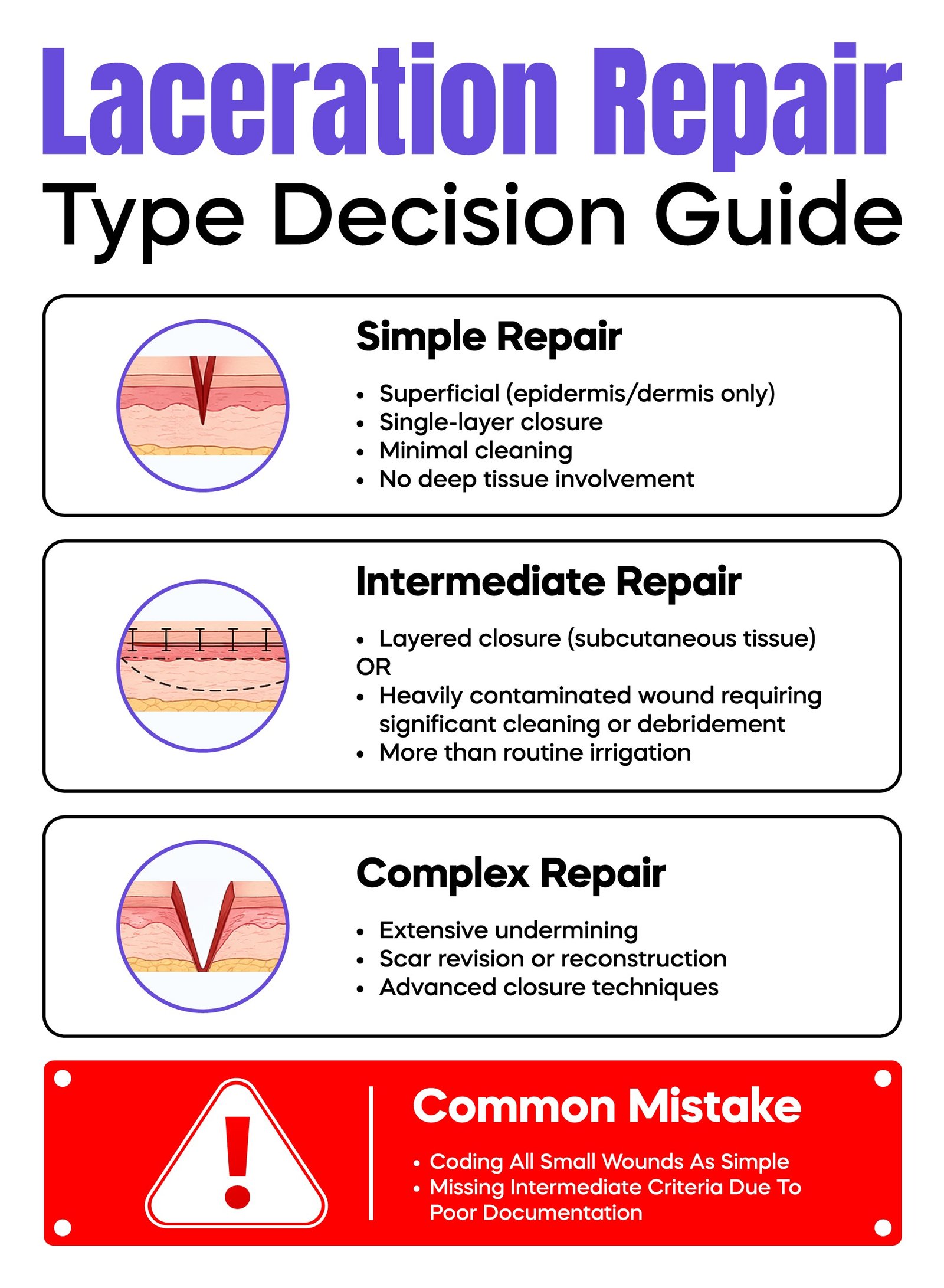
Correct classification depends on depth and work performed.
Simple repair involves a single-layer closure of superficial tissue.
Intermediate repair involves layered closure of deeper tissue, such as subcutaneous layers, or wounds that require significant debridement due to heavy contamination. Routine cleaning alone does not qualify as intermediate repair.
Complex repair involves advanced techniques such as extensive undermining or reconstruction.
A common mistake is defaulting all minor wounds to CPT 12001. This leads to undercoding when documentation supports a higher-level repair.
Modifier use must be accurate and supported by documentation.
Modifier 25 is used when a separate Evaluation and Management (E/M) service is performed on the same day as the procedure. The E/M must be significant and separately identifiable.
For example, if a patient presents with a laceration and also requires evaluation for a concussion or infection, an E/M service may be billed with modifier 25.
Modifier 59 may be used in rare cases when a separate and distinct procedural service is performed that is not normally reported together.
Modifier 24 is used when a patient returns during the 10-day global period for an unrelated issue. This allows billing of an E/M service that is not connected to the original procedure.
Incorrect or routine use of modifiers is a common audit trigger.
Tissue adhesive is commonly used in simple wound repair. Many commercial payers allow CPT 12001 when an adhesive is used as the sole method of closure.
Medicare rules are more complex. Depending on the care setting and local Medicare Administrative Contractor (MAC) guidance, adhesive-only closure may require HCPCS code G0168 or may be bundled into the E/M service.
This variation creates compliance risk. Billing teams must confirm payer-specific rules before submitting claims.
CPT 12001 has a 10-day global period. Routine follow-up care related to the procedure is included in the payment.
Services such as suture removal or wound checks cannot be billed separately during this period.
If a patient returns within 10 days for an unrelated issue, an E/M service may be billed using modifier 24 to indicate it is not related to the original procedure.
Understanding global period rules helps prevent unnecessary denials.
Denials are usually caused by preventable documentation or coding errors.
Missing wound length is the most common issue. Without measurement, the code cannot be supported.
Incorrect code selection is another problem. Using CPT 12001 for wounds larger than 2.5 cm leads to denial or downcoding.
Modifier misuse, especially with modifier 25, can result in claim rejection.
Bundling errors occur when services included in the procedure are billed separately.
Practices should review denial reports regularly and correct patterns early.
Even though CPT 12001 is a low-value code, repeated misuse can trigger audits.
Payers look for consistency between documentation and billing. Missing or vague details increase audit risk.
Overcoding creates compliance exposure. Undercoding leads to lost revenue.
Regular internal audits and staff training reduce both risks.
Providers should measure and document wound length immediately after repair.
EHR templates should require key elements such as size, location, and repair type. Templates should not allow vague entries.
Billing teams should confirm documentation supports the selected code.
Training and routine audits improve accuracy and reduce denials.
Small workflow improvements can lead to consistent revenue gains.
CPT 12001 may appear simple, but accurate billing depends on small details that are often missed in busy clinical settings. Wound size must be measured and documented clearly. Repair type must match the actual work performed. Multiple wounds must be combined correctly. These steps directly impact reimbursement and compliance.
Most denials linked to CPT 12001 are preventable. They usually come from missing measurements, incorrect code selection, or improper modifier use. Over time, even small errors can lead to consistent revenue loss or increased audit risk.
A reliable workflow makes the difference. When providers document accurately at the point of care, and billing teams verify code support before submission, claim quality improves. Practices that review denial patterns and train staff regularly see better payment outcomes and fewer compliance issues.
For physicians, the goal is not just correct coding. It is protecting the value of the care already delivered.
Arj Fatima is a senior medical billing and coding specialist with hands-on experience in U.S. healthcare reimbursement. She works closely with physicians and practice owners to improve coding accuracy, reduce denials, and maintain compliance with Medicare and commercial payer rules. Her expertise includes CPT coding, documentation audits, and revenue cycle management. She focuses on practical solutions that help doctors protect revenue and avoid billing mistakes.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

