Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us
Many physicians provide appropriate care, perform a minor procedure during the visit, and later discover the office visit was denied. The payer bundles the Evaluation and Management service into the procedure. In some cases, records are requested months after payment. This creates revenue loss and audit stress.
Modifier 25 exists to prevent that bundling when it is clinically justified. However, it is closely monitored by commercial insurers and the Centers for Medicare & Medicaid Services. It must be applied carefully and documented clearly. Used correctly, it protects revenue. Used loosely, it increases audit exposure.
This guide explains when to use Modifier 25, when not to use it, and how to defend it.
Modifier 25 is appended only to an Evaluation and Management service code. It is never attached to the procedure code.
E/M codes are part of the CPT code set maintained by the American Medical Association.
When you append Modifier 25 to the E/M code, you are telling the payer that you provided a significant and separately identifiable evaluation on the same day as a minor procedure.
Minor procedures already include a small amount of evaluation work. For example, confirming the injection site before a joint injection is included in the procedure payment. That basic assessment cannot be billed separately.
Modifier 25 applies only when your evaluation goes beyond that inherent procedural work.
Payers use automated claim-editing systems to prevent what they consider duplicate billing. For Medicare claims, bundling is largely driven by National Correct Coding Initiative edits, commonly known as NCCI edits.
NCCI edits to link certain services together. When an E/M service and a minor procedure are billed on the same day without Modifier 25, the E/M service is typically bundled into the procedure and denied.
Modifier 25 signals that the E/M service should not be bundled because it was medically necessary and separate.
If the modifier is missing, the system assumes the evaluation was routine and included in the procedure payment.
Under CPT rules, different diagnosis codes are not required when billing an E/M service with Modifier 25 and a same-day procedure.
However, many commercial payers apply proprietary edits. These systems may flag claims when the same diagnosis code is linked to both the E/M service and the procedure.
This does not make the claim incorrect under CPT standards. But it may increase denial risk depending on the payer.
From a compliance perspective, the key requirement is separate medical necessity and distinct documentation.
From a practical revenue perspective, when clinically appropriate, linking different diagnoses can reduce payer friction.
Practices should monitor denial trends by payer and adjust claim-linkage strategies accordingly.
The phrase “significant and separately identifiable” determines whether your claim survives review.
Significant means the evaluation required real medical decision-making. It was not brief, routine, or limited to preparing for the procedure.
Separately identifiable means the documentation clearly shows a distinct evaluation. If an auditor removes the procedure note, the E/M service should still stand on its own.
The E/M portion must include its own history, exam elements when relevant, and documented medical decision-making beyond procedural planning.
If the evaluation simply leads directly to the procedure without additional assessment, Modifier 25 is not appropriate.
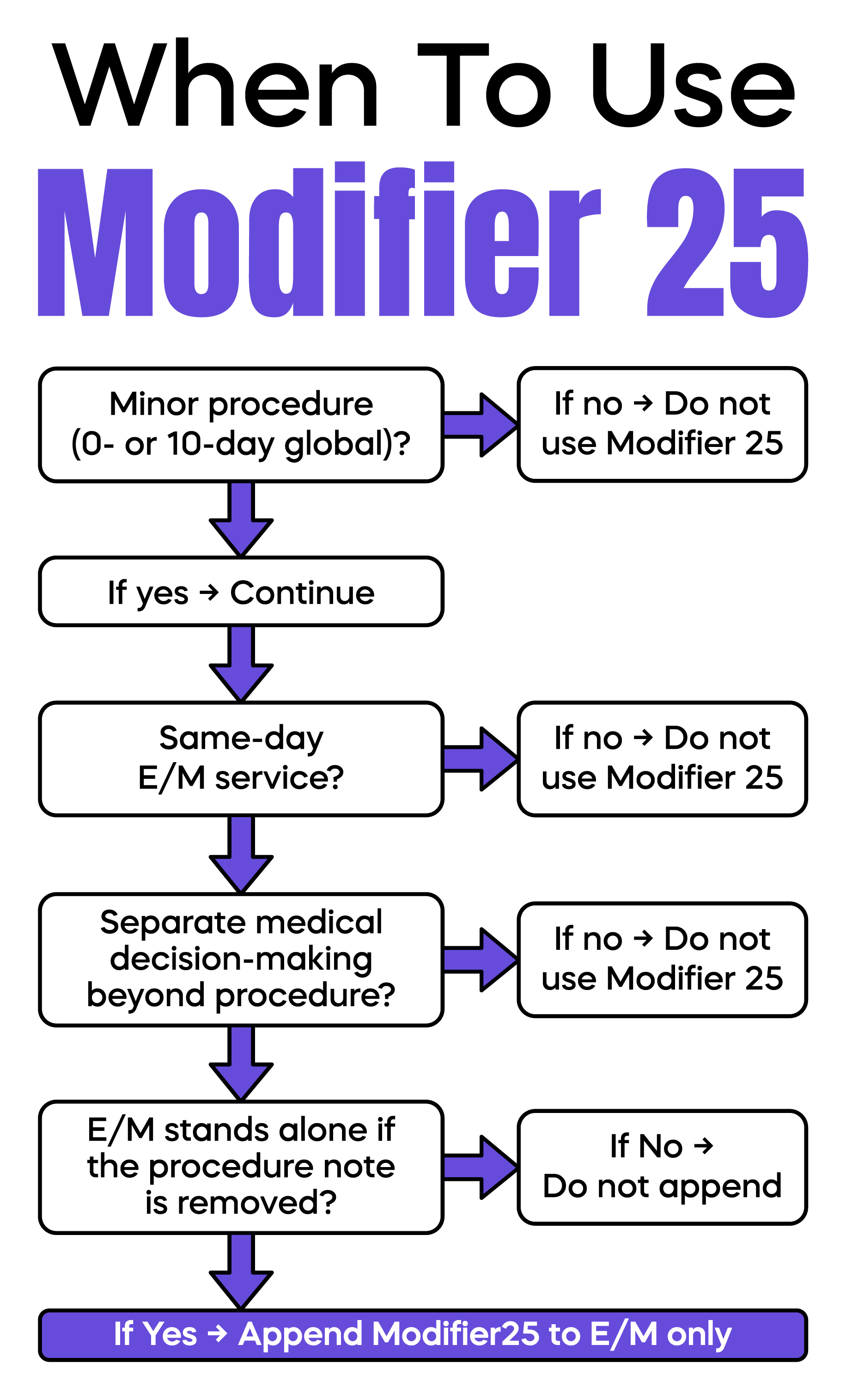
Modifier 25 is appropriate when three conditions exist.
A minor procedure is performed.
An E/M service occurs on the same day.
The E/M service is medically necessary and distinct from the procedure.
Consider a primary care example.
A patient presents for diabetes follow-up. Labs are reviewed. Medication is adjusted. During the visit, the patient reports a painful abscess. You evaluate the abscess and perform incision and drainage.
The diabetes management supports the E/M service. The drainage is the procedure. Modifier 25 is appended to the E/M code only.
In dermatology, a patient presents for evaluation of multiple suspicious lesions due to prior melanoma. You perform a full skin exam and decide to biopsy one lesion. The comprehensive evaluation supports an E/M service. The biopsy is separately reportable.
In urgent care, a patient presents with ankle pain but also reports new shortness of breath. You evaluate both problems and perform an ankle injection. If the respiratory evaluation required separate medical decision-making, Modifier 25 may be appropriate.
Modifier 25 may be used on the same date as a preventive medicine service, but only under strict conditions.
Preventive codes such as 9938x or 9939x cover routine annual exams. They do not include evaluation of new or worsening problems that require additional medical decision-making.
If, during the preventive visit, you evaluate and manage a separate medical issue requiring problem-oriented medical decision-making, you may bill a separate E/M code such as 99213–99215.
Modifier 25 is appended only to the problem-oriented E/M code, never to the preventive code.
Documentation must clearly separate the preventive service from the problem-oriented E/M service. The history, assessment, and plan for the problem must stand alone.
This is a common audit focus area. Blended documentation often results in the denial of the problem-oriented E/M service.
Modifier 25 is not appropriate when the evaluation is minimal and directly related to performing the procedure.
If a patient schedules a visit only for wart removal and you confirm the site and remove it, that brief evaluation is included in the procedure payment.
If documentation does not clearly support separate medical decision-making, do not append the modifier.
Routine use of Modifier 25 on every procedure visit is a compliance risk. Payers track utilization patterns. Outliers often face prepayment review.
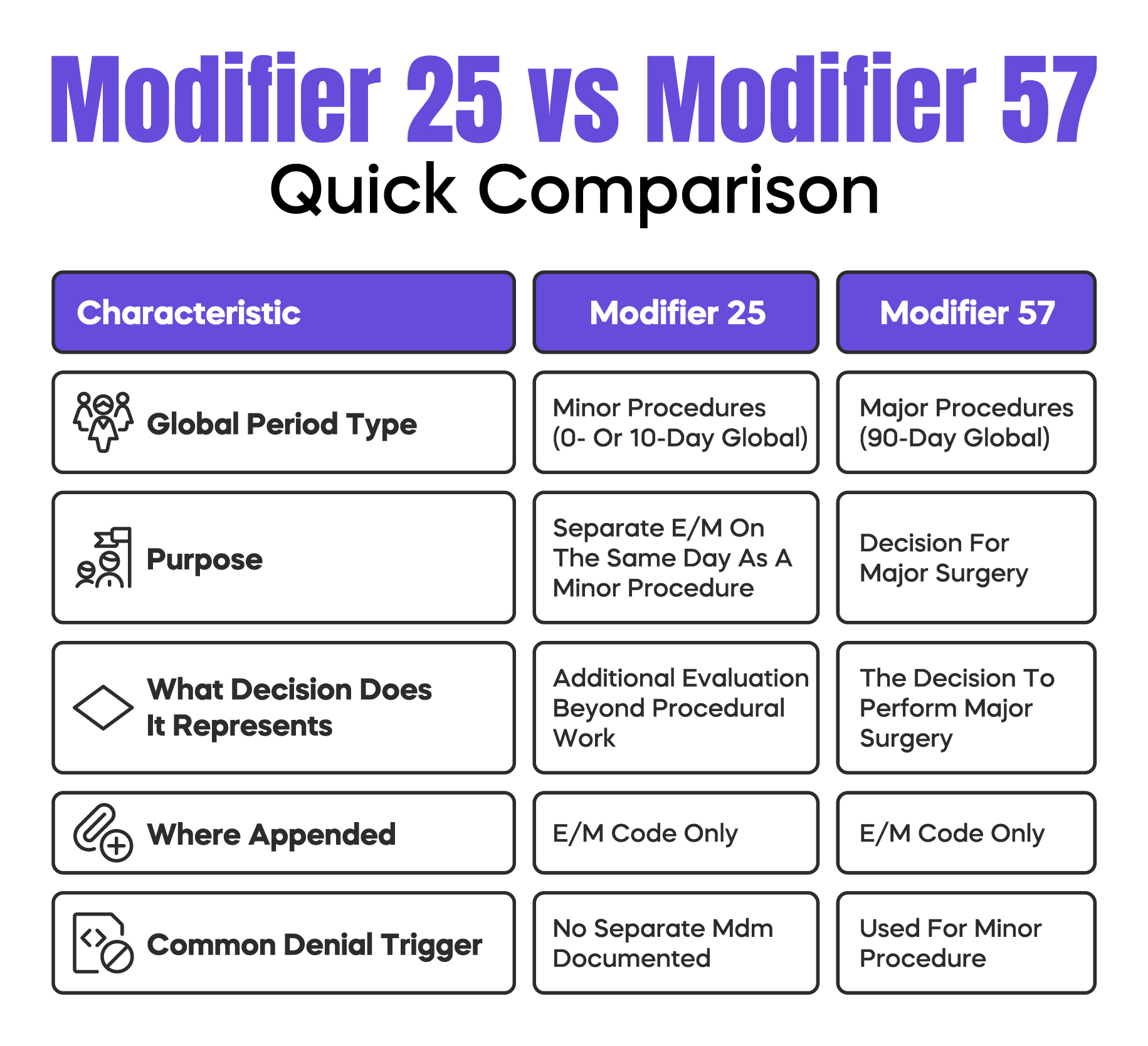
Most minor procedures have a 0-day or 10-day global period. The global period means related services on that day and shortly after are included in the procedure payment.
Modifier 25 applies only to same-day E/M services tied to minor procedures.
It should not be confused with Modifier 57, which applies when the decision is made to perform a major surgery with a 90-day global period.
Using the wrong modifier leads to immediate denial.
Knowing the global period for your commonly billed CPT codes reduces preventable errors.
Strong documentation is the foundation of Modifier 25 compliance.
Your note should include a clear chief complaint that supports the evaluation. It should document history and exam elements relevant to the separate issue. It must show medical decision-making beyond procedural planning.
The procedure should be documented in a clearly separated section.
A practical test is simple. If an auditor deletes the procedure portion of your note, the E/M service should still appear complete and medically necessary.
Avoid cloned language across multiple encounters. Repeated identical notes associated with Modifier 25 increase scrutiny.
Modifier 25 increases reimbursement when properly applied. For that reason, it is closely monitored.
Common denial triggers include high-level E/M codes paired with simple procedures, insufficient documentation, and excessive utilization rates compared to peers.
If one physician appends Modifier 25 to 60 percent of minor procedures while others average 15 percent, that provider may trigger review.
Internal auditing and periodic education reduce this risk.
Modifier 25 is not a billing tactic. It is a compliance mechanism that allows accurate reporting of legitimate evaluation work performed on the same day as a minor procedure.
Append it only to the E/M code. Use it when the evaluation stands on its own. Separate your documentation clearly. Monitor internal utilization patterns. Understand how bundling edits affect your specialty.
Disciplined use protects both revenue and professional integrity.
Arj Fatima is a U.S. medical billing and compliance content specialist with hands-on experience in physician revenue cycle workflows, payer audits, CPT coding interpretation, and documentation risk analysis. She writes for private practices, solo physicians, and specialty groups across the United States, focusing on practical billing accuracy, denial prevention, and audit readiness strategies.
Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.