Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


For cardiologists and practice owners, coding patients with both hypertensive heart disease and chronic kidney disease (CKD) can be challenging. Mistakes often lead to claim denials, audit risk, and lost revenue. Many practices code heart failure and CKD separately, but ICD-10-CM guidelines presume these conditions are linked unless the provider documents otherwise. Insurance payers expect the use of combination codes from the I13 category, which reflect the causal relationship between hypertension, heart disease, and CKD. Knowing the difference between ICD-10 I13.0 and I13.2 and how to sequence them is critical for accurate documentation and reimbursement.
ICD-10-CM coding guidelines rely on the word “with” to indicate a presumed causal relationship. When a patient has hypertension and CKD, or hypertension and heart disease, the guidelines assume the hypertension has caused organ damage. The physician does not need to explicitly state this. Unless the record documents that the conditions are unrelated, coders should use I13 combination codes instead of separate I11 (hypertensive heart disease) and I12 (hypertensive CKD) codes. This prevents underreporting complexity and reduces audit risk.
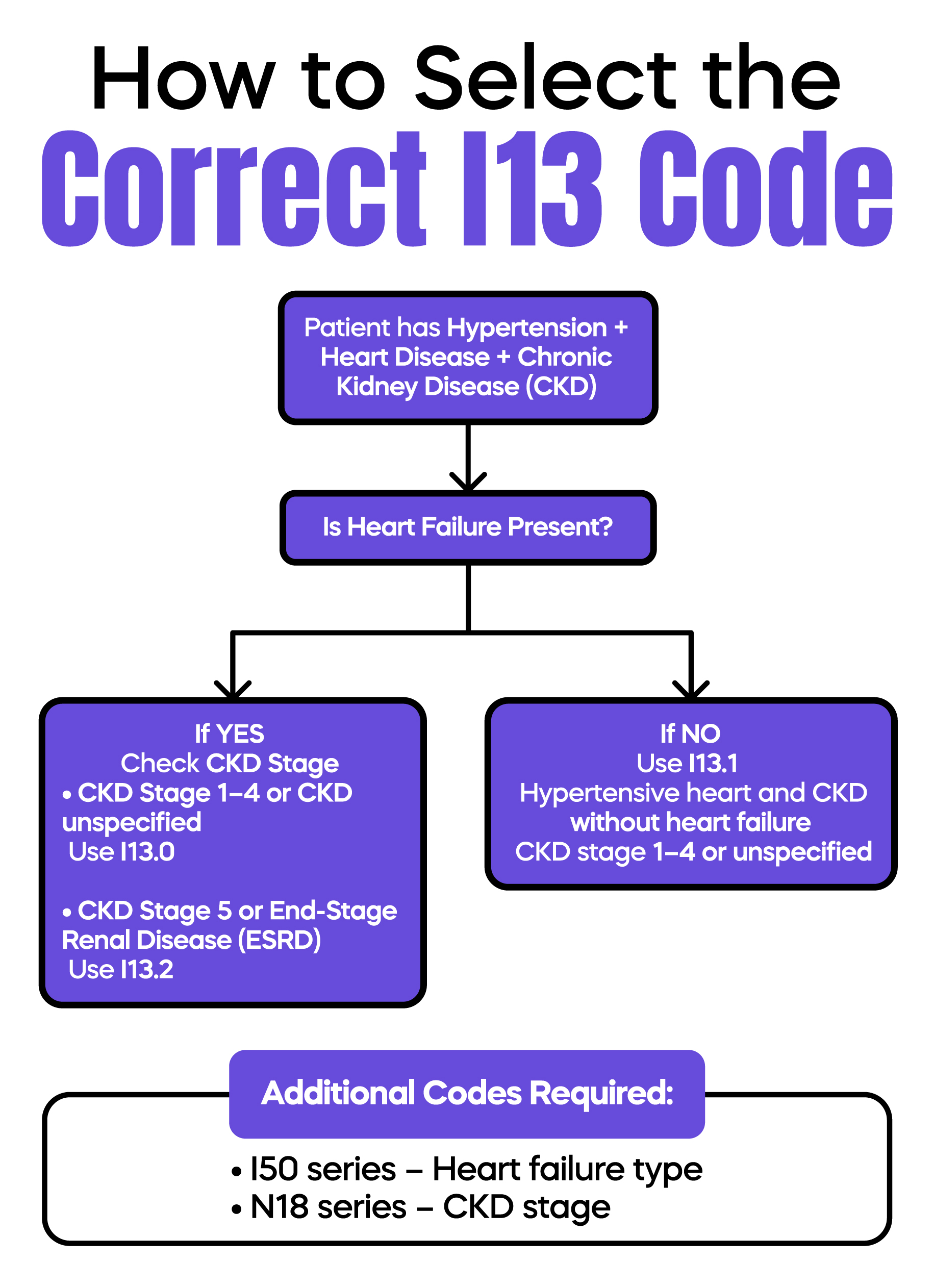
The I13 category covers hypertensive heart disease and chronic kidney disease. Heart involvement may or may not include heart failure, depending on the code. The category is divided as follows:
I13.0 – Hypertensive heart and CKD with heart failure and CKD stage 1–4 or unspecified stage.
I13.1 – Hypertensive heart and CKD without heart failure, CKD stage 1–4 or unspecified stage.
I13.2 – Hypertensive heart and CKD with heart failure and CKD stage 5 or End-Stage Renal Disease (ESRD).
Correct code selection ensures that the claim reflects the patient’s true clinical complexity. Using I13.1 is appropriate when heart failure is absent, which is important for both documentation and reimbursement.
The choice between I13.0 and I13.2 depends entirely on the CKD stage.
I13.0 is used when heart failure is present, and CKD is stage 1–4 or unspecified.
I13.2 is used when heart failure is present, and CKD has progressed to stage 5 or ESRD.
Selecting the wrong code can misrepresent patient complexity and affect reimbursement. CKD unspecified stage is included under I13.0, which is useful when the exact stage is not documented, but heart failure is present.
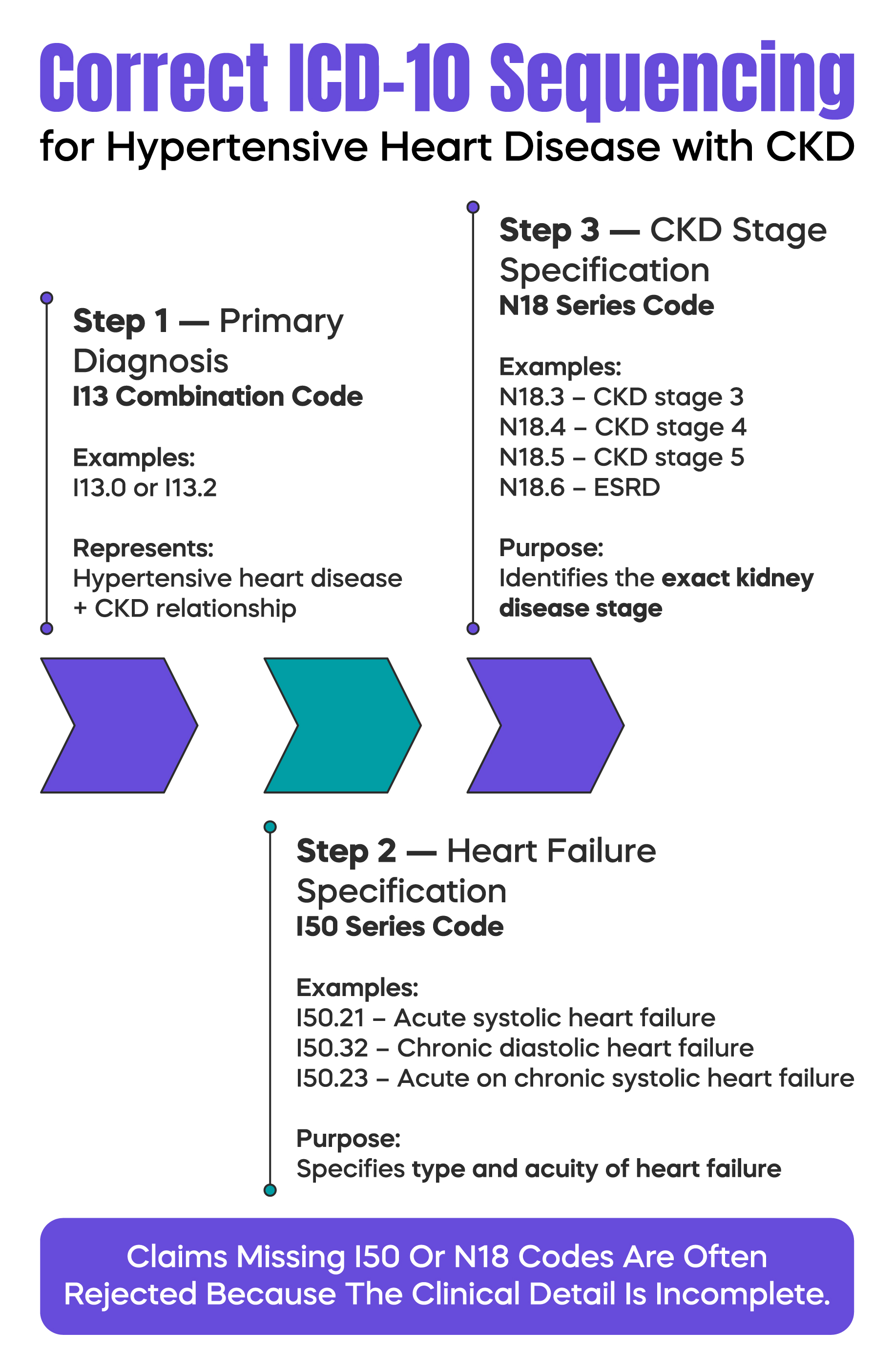
I13 combination codes require secondary codes for full clinical specificity.
Heart failure: Use the I50 series to indicate type and acuity. Examples include I50.21 for acute systolic heart failure, I50.32 for chronic diastolic, and I50.23 for acute on chronic systolic.
CKD stage: Use the N18 series to specify the stage. For I13.0, use N18.1–N18.4 or N18.9 if unspecified. Stage 3 may require N18.30 (stage 3), N18.31 (stage 3a), or N18.32 (stage 3b). For I13.2, use N18.5 for stage 5 or N18.6 for ESRD.
Without these secondary codes, the claim is incomplete, which can trigger denials or downcoding. Accurate coding also affects risk adjustment and Medicare reporting.
Proper sequencing ensures compliance with ICD-10 manifestation logic:
Following this order reduces denials and demonstrates the clinical rationale for the visit and procedures provided.
One frequent mistake is unbundling hypertension by coding I10 separately, along with heart and kidney disease. This violates ICD-10 rules because I13 already includes the hypertension component.
Another common error is vague documentation, such as stating “heart failure” without specifying systolic, diastolic, acute, or chronic. This prevents accurate selection of I50 secondary codes, leading to incomplete claims and downcoding.
To justify coding and support audits, documentation should include:
Incomplete documentation can prevent the correct use of I13 codes and increase payer scrutiny.
ICD-10 I13.0 and I13.2 allow precise documentation of hypertensive heart disease with CKD and heart failure. Selecting the correct code, adding secondary codes for heart failure and CKD stage, and sequencing codes properly protects revenue and reduces audit risk. Following these guidelines ensures claims accurately reflect clinical complexity and comply with ICD-10-CM rules.
Arj Fatima is a U.S. medical billing expert with experience in cardiology and primary care practices. She specializes in ICD-10-CM compliance, revenue cycle management, and audit prevention strategies. Her work focuses on helping physicians improve documentation accuracy, reduce denials, and optimize reimbursement.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

