Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us
Many physicians discover a missing authorization only after a claim is denied. The service was necessary. The documentation was written. The patient was treated appropriately. Yet payment stops because prior approval was not on file.
Retro Authorization becomes the recovery mechanism.
Retro Authorization means requesting approval from an insurance payer after a medical service has already been performed. It is used when prior authorization was not obtained before treatment.
It is not routine. It is considered an exception. Approval depends on timing, documentation, medical necessity, and payer policy.
Retro Authorization directly affects revenue stability.
When claims are denied for missing authorization, cash flow slows. Accounts receivable increase. Staff time shifts from proactive billing to denial management. Small practices feel this impact quickly, especially when high-cost imaging or procedures are involved.
It also affects compliance risk.
Frequent authorization failures may signal weak front-end processes. Commercial payers and Medicare Advantage plans monitor patterns. Repeated issues can trigger pre-payment review or focused audit activity through contractors such as Medicare Administrative Contractors, Unified Program Integrity Contractors, or Recovery Audit Contractors operating under the oversight of the Centers for Medicare & Medicaid Services.
Retro Authorization protects revenue in isolated cases. It does not replace strong Revenue Cycle Management systems.
Understanding terminology prevents billing errors.
Prior authorization means payer approval is required before a service is performed. If approval is not obtained in advance, the claim may be denied.
Pre-authorization is typically used interchangeably with prior authorization by commercial payers. In most cases, there is no operational difference. Both require approval before treatment.
Retro Authorization is requested after the service has already occurred. It asks the payer to approve the service after the fact because prior approval was not secured.
The difference is timing. Prior and pre occur before care. Retro occurs after care.
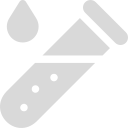
The most common reason is clinical urgency.
If a patient presents with unstable symptoms, treatment cannot wait for portal approval. In emergencies, documentation must clearly show that a delay would have risked harm.
Another common reason is insurance eligibility confusion. A patient may provide outdated insurance information. Coverage may change mid-month. The practice bills the wrong payer and discovers the issue after denial.
In surgical settings, intraoperative findings may require additional procedures beyond what was originally planned. The surgeon cannot pause surgery to request expanded authorization.
Administrative errors also occur. However, payers are less forgiving when the delay results from internal staff oversight.
Not every case qualifies for retro review.
Eligibility depends on:
The payer’s specific policy.
Whether the delay was emergent or administrative.
Whether the request is submitted within the payer’s deadline.
Whether the patient’s benefit plan allows retro approval.
Commercial plans often allow retro requests only within 24 to 72 hours for emergency admissions. Some allow up to 14 days for documented extenuating circumstances. Others deny retro approval entirely for non-emergency services.
Traditional Medicare under the Centers for Medicare & Medicaid Services does not require prior authorization for most physician services. However, select services are subject to prior authorization under specific CMS programs such as the Outpatient Department Prior Authorization Program and certain Durable Medical Equipment categories billed under HCPCS codes.
Medicare Advantage plans frequently impose broader prior authorization requirements and stricter retro policies.
The process begins after a denial for missing authorization or when staff realizes authorization was not obtained.
First, confirm whether the payer allows retro approval for that plan.
Second, review the payer’s deadline. Time windows are strict.
Third, assemble the full medical record for the date of service.
Fourth, submit the retro request through the payer portal or provider services channel.
Fifth, monitor for response and follow up promptly. Retro requests usually require manual clinical review.
If denied, the case may proceed to formal appeal or peer-to-peer review.
A strong retro request includes complete clinical support.
The documentation must show medical necessity. Medical necessity means the service was reasonable, appropriate, and aligned with accepted standards of care.
Procedure codes under CPT must align clearly with diagnosis codes under ICD-10-CM. If the diagnosis does not justify the procedure, approval is unlikely.
Most retro packets should include:
Signed progress notes.
History of present illness.
Failed conservative treatment history when applicable.
Diagnostic imaging or lab findings.
Clear explanation of urgency or extenuating circumstance.
Payers may evaluate documentation against coverage criteria described in National Coverage Determinations and Local Coverage Determinations.
If documentation does not meet those standards, the request will likely fail.
The most common reason is weak documentation.
Brief notes without clear urgency are often labeled elective.
Missing payer deadlines is another frequent cause. Even one day late can result in denial.
Coding inconsistencies between requested procedures and billed services also trigger rejection.
Some benefit plans explicitly exclude retro approvals. In those cases, no documentation can override the contract.
If the retro request fails, you may pursue a formal appeal.
A peer-to-peer review allows the treating physician to speak directly with the payer’s medical director. This often clarifies clinical nuance that written documentation cannot fully capture.
If necessary, escalate to higher-level appeals. Maintain records of all conversations and reference numbers.
Financial responsibility depends on payer contract terms and patient financial agreements.
Repeated retro authorization issues may indicate systemic workflow problems.
Oversight does not occur through direct CMS surveillance of individual providers. Instead, utilization review and payment oversight typically occur through Medicare Administrative Contractors, Unified Program Integrity Contractors, Recovery Audit Contractors, and Medicare Advantage plan-level utilization management programs operating under the oversight of the Centers for Medicare & Medicaid Services.
If authorization failures become frequent, practices should conduct internal audits. Identify workflow breakdowns. Implement corrective action. Documentation of corrective measures demonstrates a compliance effort if reviewed.
Prevention is more effective than correction.
Verify insurance eligibility and authorization requirements before services are scheduled whenever possible.
Do not schedule high-cost imaging, surgeries, or specialty treatments without documented authorization unless the situation is emergent.
For emergency admissions, assign a staff member to notify payers within the required timeframes.
Retro Authorization should remain rare. When it becomes routine, it signals weakness in front-end billing controls.
Retro Authorization is a request to an insurance payer to approve a medical service after it has already been performed. It is typically allowed only in emergencies, sudden eligibility changes, or documented extenuating circumstances. Approval depends on strict deadlines, strong medical necessity documentation, correct CPT and ICD-10-CM coding alignment, and payer-specific policies. Effective front-end authorization processes are the best protection against revenue loss.
Arj Fatima is a Senior Revenue Cycle Strategist with over 10 years of experience helping U.S. medical practices navigate payer bureaucracy. She specializes in specialty-specific coding and denial recovery, ensuring that physicians are fairly compensated for the care they provide. Her work focuses on bridging the gap between clinical excellence and administrative compliance.
Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.