Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us
For U.S. physicians, a "pending" claim is more than an administrative delay; it is a direct hit to the practice's liquidity. In a landscape governed by the Centers for Medicare & Medicaid Services (CMS) and complex commercial contracts, behavioral health providers face unique hurdles. Unlike other specialties, mental health reimbursement depends heavily on time-based coding and highly subjective medical necessity standards.
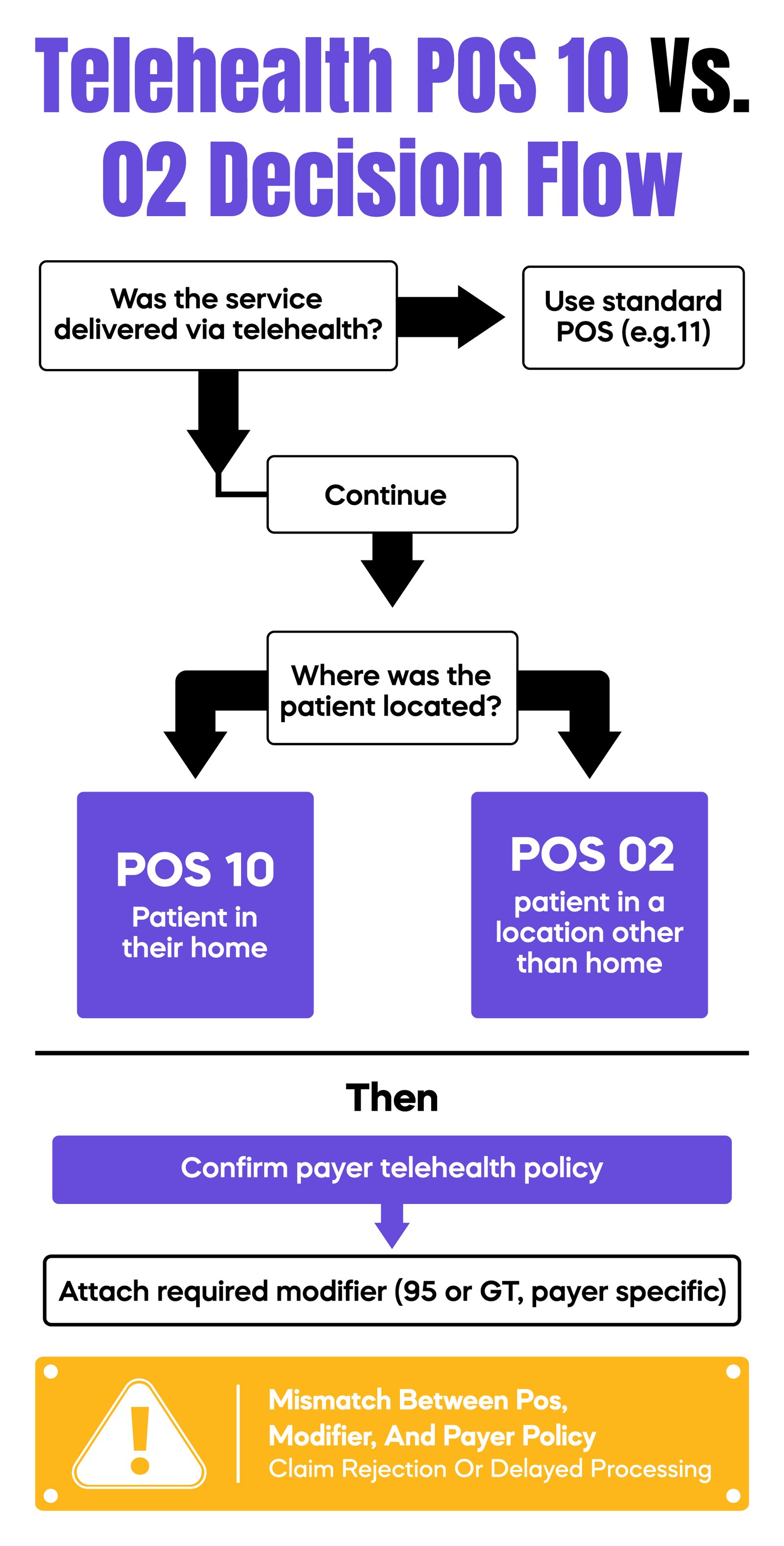
To achieve a "Clean Claim Rate" above 95%, you must understand the invisible barriers within the Revenue Cycle Management (RCM) process. Below are the ten primary structural causes for payment delays and how to bypass them.
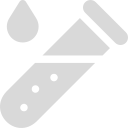
CPT code 90837 (psychotherapy, 60 minutes) is often the highest-reimbursed service in an outpatient setting, making it a prime target for payer scrutiny. Most Medicare Administrative Contractors (MACs) and commercial payers use automated algorithms to flag providers who bill 90837 more than 50% of the time. When you exceed this frequency threshold, the payer triggers a "Pre-Payment Review." This is not a denial, but it halts the payment clock while they request clinical documentation. To avoid this, notes must demonstrate complexity—detailing risk assessments, specific therapeutic interventions like DBT or CBT, and why a standard 45-minute session (90834) would have been insufficient for the patient’s clinical goals.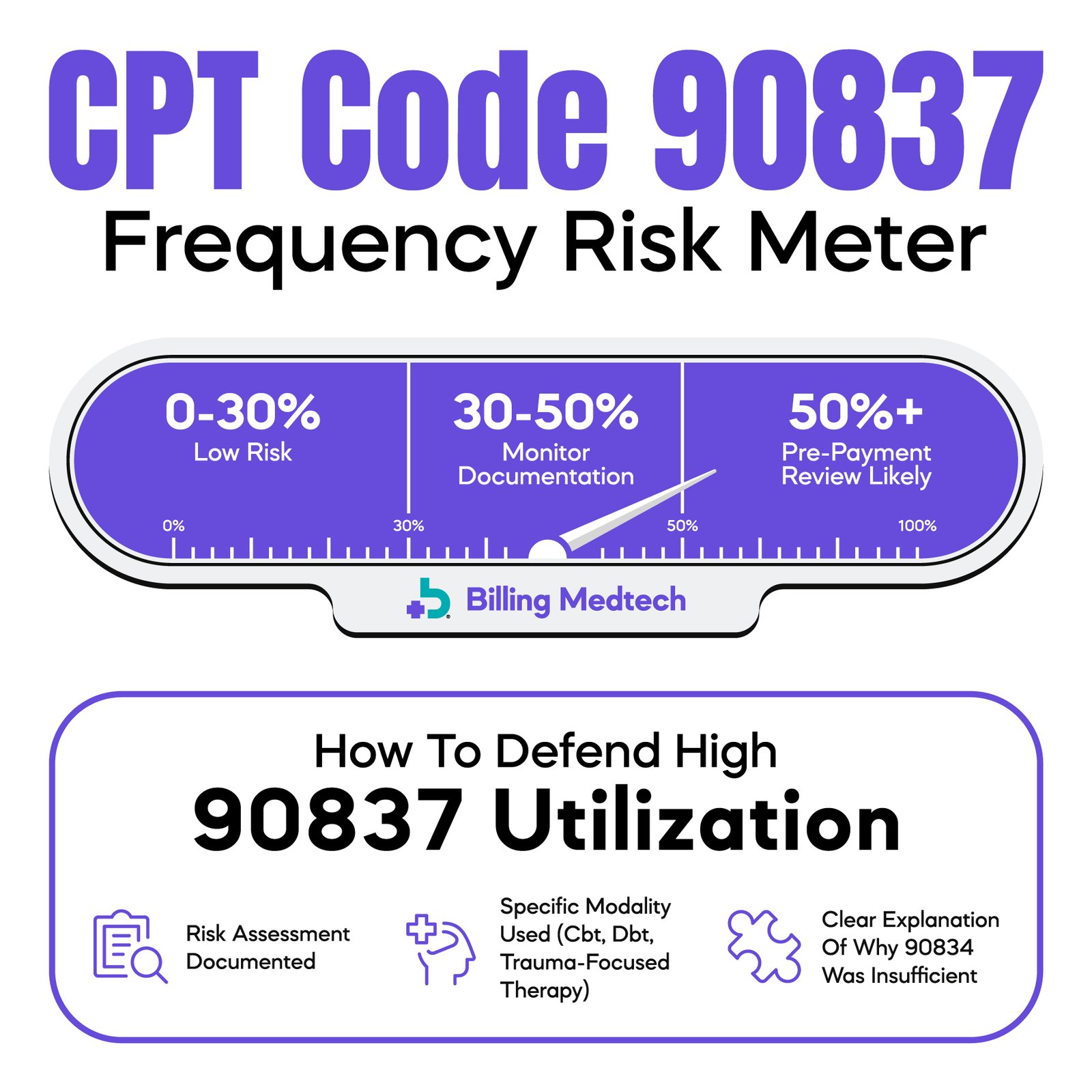
Post-pandemic telehealth regulations have become increasingly rigid. A common operational failure is the use of an incorrect Place of Service (POS) code. If your patient is receiving services at home, POS 10 must be used; for other locations, POS 02 applies. When these codes are paired with a "95" modifier but documented in an office setting (POS 11), the claim fails the "Front-End Edit" at the clearinghouse or payer level. This creates a technical rejection that requires manual intervention, often delaying reimbursement by 30 days or more as the claim is corrected and resubmitted.
Behavioral health patients often experience transitions in employment or Medicaid status, leading to "eligibility volatility." If your practice does not perform real-time eligibility (RTE) verification at every encounter, you risk billing inactive policies. Payer databases often lag; a patient may appear active on a portal but be terminated on the backend. This leads to a "Member Not Found" rejection. By the time the front office gathers new insurance information, the "Timely Filing" limit, which can be as short as 60 to 90 days for some commercial payers, may have already passed.
When a new provider joins a group, they enter a "credentialing shadow period." Even if the provider has an active NPI, they may not be "linked" to your group’s Tax ID in the payer’s system. Submitting claims during this window results in a "Provider Not Contracted" denial. In some jurisdictions, payers will "pend" these claims indefinitely rather than denying them, leaving you without a clear path to appeal. Practices must verify "par status" for every new clinician before scheduling their first billable session to prevent an unrecoverable backlog of aging Accounts Receivable (AR).
Coordination of Benefits remains a leading cause of "silent" payment delays. When a patient has dual coverage, the primary payer may withhold payment until the patient confirms that no other insurance is primary. This is often used as a stalling tactic by payers. As the provider, you cannot resolve this on the patient’s behalf. If your billing team doesn't identify this delay within the first 14 days, the claim can sit in "Pending" status for months. Implementing a policy where patients must verify COB during intake is essential for maintaining steady cash flow.
Payers are now utilizing Natural Language Processing (NLP) to perform "Desk Audits" on a massive scale. These AI filters look for "cloned notes" documentation that is significantly similar from one session to the next. In behavioral health, where progress can be incremental, cloned notes are often flagged as evidence of "lack of medical necessity" or "maintenance care." When the AI detects a pattern of repetitive text, it triggers a manual audit of the entire patient file, freezing all related payments until a human reviewer confirms the services were distinct and restorative.
The recent alignment of 42 CFR Part 2 with HIPAA has introduced new electronic data interchange (EDI) requirements. For practices treating Substance Use Disorders (SUD), claims must be transmitted with specific privacy indicators. If a claim containing an SUD-related ICD-10 code is sent without the "Consent on File" flag (Loop 2300 in the 837P file), payers will automatically reject the claim to prevent a breach of federal privacy laws. Ensuring your Electronic Health Record (EHR) system is updated to handle these specific 2026 compliance headers is non-negotiable for SUD providers.
Many intensive behavioral health services, such as Partial Hospitalization Programs (PHP) or Intensive Outpatient Programs (IOP), require Prior Authorization. A common failure point is "unit exhaustion," where a practice continues treatment beyond the authorized number of sessions. Payers rarely provide "low balance" alerts. Once the authorized units are consumed, the system denies subsequent claims as "No Authorization on File." Managing this requires a dedicated "Authorization Tracker" within your RCM workflow to trigger re-authorization requests at least three sessions before the current PA expires.
The National Correct Coding Initiative (NCCI) establishes which codes can be billed together. In behavioral health, billing an Evaluation and Management (E/M) code alongside a psychotherapy add-on (e.g., 90833) requires Modifier 25 or 59, depending on the payer. However, overuse of Modifier 59 to bypass "CCI edits" is a high-risk audit trigger. Payers often delay these "unbundled" claims to verify that the two services were truly separate and not part of a single session. Incorrect use of these modifiers is a primary cause of partial payment or "Line Item Denials."
Before a claim reaches the insurance company, it must pass through the clearinghouse "scrubber." If there is a "front-end" error, such as an invalid NPI, a missing 9-digit zip code, or an incorrect subscriber ID, the claim is "rejected," not denied. This means it never enters the payer’s system. Many practices fail to monitor their "Rejection Reports" daily, assuming that "submitted" means "received." Claims sitting in a rejected state do not count toward timely filing deadlines, often resulting in a total loss of revenue if not caught within 24–48 hours.
In the current U.S. healthcare climate, behavioral health physicians cannot afford to treat Revenue Cycle Management as an afterthought. As we have explored, payment delays are rarely the result of a single error; they are the cumulative effect of shifting regulatory landscapes, payer-specific AI filters, and front-end operational gaps.
By addressing the "Top 10" triggers, from the 90837 frequency trap to the nuances of 42 CFR Part 2, you transition your practice from a reactive state of chasing denials to a proactive state of revenue protection. The goal is to achieve a Clean Claim Rate of 95% or higher, ensuring that your focus remains where it belongs: on patient outcomes rather than administrative friction.
Arj Fatima is a senior Revenue Cycle Management (RCM) strategist with 10+ years of expertise in U.S. behavioral health billing. Specializing in compliance and the No Surprises Act, she helps solo practitioners and large groups recover lost revenue by identifying "leaks" in the billing cycle. Arj simplifies complex billing jargon into actionable paths to full reimbursement, ensuring physicians focus on patients, not paperwork.
Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.