Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Joint replacement surgeries improve mobility. But from a billing standpoint, they carry high financial risk. Total hip and total knee arthroplasties are closely reviewed by payers because they are high-cost procedures. A small documentation gap can delay payment or trigger an audit.
When a claim includes CPT 27130 or CPT 27447 on the CMS-1500 form, payers immediately review medical necessity, diagnosis linkage, modifiers, and global compliance. If any element is unclear, reimbursement may be denied or reduced.
This guide explains CPT 27130 vs 27447 from a U.S. medical billing and compliance perspective, with precise clarification based on CMS policy and common MAC review standards.
CPT 27130 represents total hip arthroplasty. This means complete replacement of the hip joint using prosthetic components.
To correctly report 27130, both of the following must be documented:
The acetabular component, which is the socket portion of the pelvis, must be prepared and replaced.
The femoral component, including the femoral stem and head, must also be inserted.
If only the femoral head is replaced, such as in a hemiarthroplasty, CPT 27130 is not appropriate. In those cases, CPT 27125 is typically used. Reporting a total replacement code for a partial procedure is a frequent audit finding under the Centers for Medicare & Medicaid Services (CMS).
Clear operative documentation must describe preparation of the acetabulum and the femoral canal, along with placement of prosthetic components. Missing one of these elements can result in denial.
Typical ICD-10-CM diagnoses linked to 27130 include:
M16.11 or M16.12 for primary osteoarthritis of the hip
M87 for avascular necrosis
M19 for secondary degenerative conditions
The diagnosis must reflect severe joint damage supported by imaging and documented functional limitation. A nonspecific pain code will not support medical necessity.
CPT 27447 represents total knee arthroplasty. This procedure involves the replacement of the distal femur and proximal tibia. Patellar resurfacing, when performed, is bundled into the procedure and is not separately billable.
For accurate reporting, documentation must show a complete joint replacement. If only one compartment of the knee is treated, such as in a unicompartmental knee replacement, 27447 cannot be used.
Reporting a total knee code for a partial procedure is an easy audit target. Payers compare the operative report to CPT code descriptors carefully.
The most common ICD-10-CM diagnoses include:
M17.11 or M17.12 for primary osteoarthritis of the knee
Other inflammatory or post-traumatic diagnoses may apply, but documentation must clearly justify full joint replacement.
The main difference between CPT 27130 vs 27447 is anatomical location. One applies to the hip. The other applies to the knee.
However, several operational differences impact reimbursement and compliance.
Relative Value Units differ under the Medicare Physician Fee Schedule. Each code has distinct work and practice expense components.
Diagnosis patterns differ. Hip replacements often involve avascular necrosis in addition to osteoarthritis. Knee replacements are most commonly performed for degenerative osteoarthritis.
Anatomical documentation focus differs. For 27130, reviewers look for confirmation of acetabular and femoral replacement. For 27447, they look for distal femur and proximal tibia replacement.
Laterality reporting is mandatory for both procedures. Most payers require RT or LT modifiers. For bilateral procedures, billing rules vary. Some payers require modifier 50. Others require two separate line items with RT and LT. Practices must verify payer-specific instructions to avoid denials.
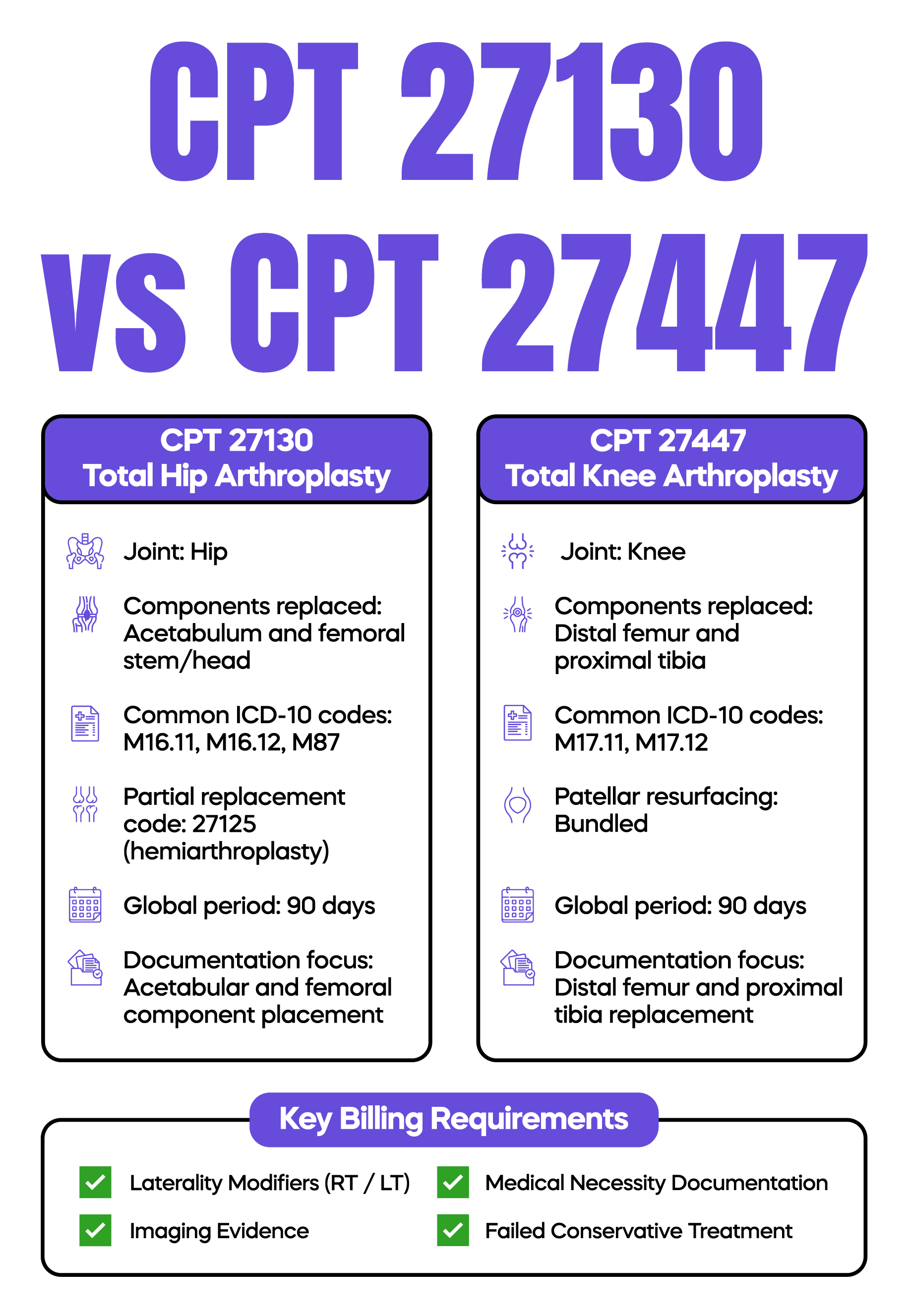
Both CPT 27130 and CPT 27447 carry a 90-day global surgical package under CMS policy.
Routine postoperative visits related to the surgery are included in the original payment. Billing separately for standard follow-up care will result in denial.
An evaluation and management service may be billed during the global period only if it is unrelated to the surgery. In that case, modifier 24 must be appended, and documentation must clearly support medical necessity.
If a staged procedure is planned, modifier 58 may apply.
Failure to apply global rules correctly is a common compliance risk in orthopedic practices.
CMS and regional Medicare Administrative Contractors review total joint claims carefully. Most Local Coverage Determinations require documentation of:
Failed conservative treatment, such as physical therapy, medication management, or injections.
Imaging evidence showing joint degeneration.
Functional limitation affecting activities of daily living.
The medical record must tell a consistent story. If the preoperative note does not summarize failed conservative care, the payer may deny the claim even if therapy records exist elsewhere in the EHR.
Reviewers compare documentation against LCD criteria line by line during audits.
The National Correct Coding Initiative establishes bundling rules. Certain services are included in total joint arthroplasty and cannot be billed separately.
For example, patellar resurfacing is bundled into CPT 27447. Attempting to report an additional code for that work may trigger a denial.
Practices should review NCCI edits regularly to prevent improper unbundling.
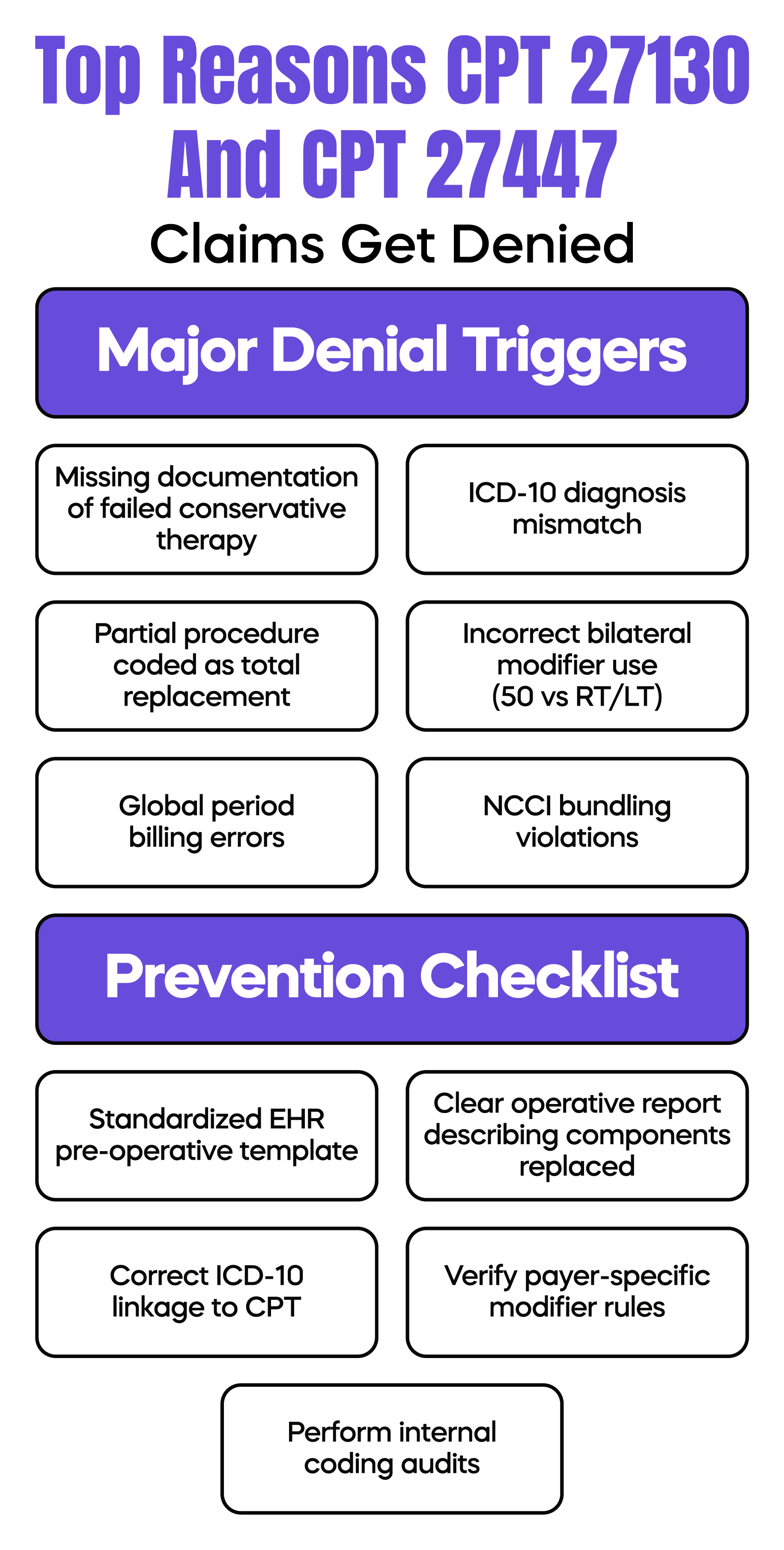
Denials for CPT 27130 and 27447 typically occur for predictable reasons.
One common issue is the lack of documentation of conservative therapy. If the chart jumps from mild symptoms to surgery without documented treatment attempts, payers may question the necessity.
Another issue is diagnosis mismatch. Linking a minor injury code to a total joint replacement will trigger automated edits at the clearinghouse level.
Incorrect bilateral reporting is also frequent. Using modifier 50 when a payer requires separate RT and LT lines can delay reimbursement.
Global period billing errors are another source of audit risk, especially when postoperative procedures are billed without confirming bundling status.
CPT 27130 vs 27447 may appear simple from a clinical standpoint. One replaces a hip. The other replaces a knee.
From a billing perspective, both codes require precise anatomical documentation, accurate ICD-10-CM linkage, proper modifier use, and strict adherence to CMS global and NCCI rules.
Consistent internal audits, structured EHR templates, and payer-specific billing verification are essential safeguards. These steps reduce denials, protect revenue, and lower audit exposure for orthopedic practices.
Arj Fatima is a U.S. medical billing and coding specialist with deep expertise in orthopedic Revenue Cycle Management, CPT compliance, CMS policy interpretation, and audit defense. She works directly with physicians and practice owners to reduce denials, strengthen documentation standards, and protect reimbursement for high-risk surgical procedures, including total hip and total knee arthroplasty.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

