Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


CPT 93306 is one of the most commonly used cardiology billing codes, yet it is also one of the most misunderstood. Many physicians perform a full echocardiogram but still face denials, downcoding, or audit risk. The issue is rarely clinical. It is almost always documentation gaps, incorrect code selection, or billing errors.
A frequent real-world problem occurs when a complete study is performed, but the report does not clearly support all required components. The payer then reduces the claim to a lower-paying code or denies it. Over time, this leads to steady revenue loss.
At the same time, this code is closely watched by Medicare and commercial payers because of its higher reimbursement. Any mismatch between what is performed and what is documented can trigger audits and clawbacks.
This guide explains CPT 93306 in simple terms. It combines clinical clarity with billing accuracy, helping physicians protect revenue and reduce compliance risk.
CPT 93306 describes a complete transthoracic echocardiogram (TTE). This is a non-invasive ultrasound of the heart performed through the chest wall.
In billing terms, this code represents a full evaluation of the heart structure and blood flow. It is not a basic scan. It is a comprehensive study that must include multiple imaging and Doppler components.
Because it is a complete study, CPT 93306 carries higher reimbursement than limited echocardiogram codes. That is why it is also a common target for audits.
The key point for physicians is simple. Performing the test is not enough. The report must clearly prove that every required component was completed.
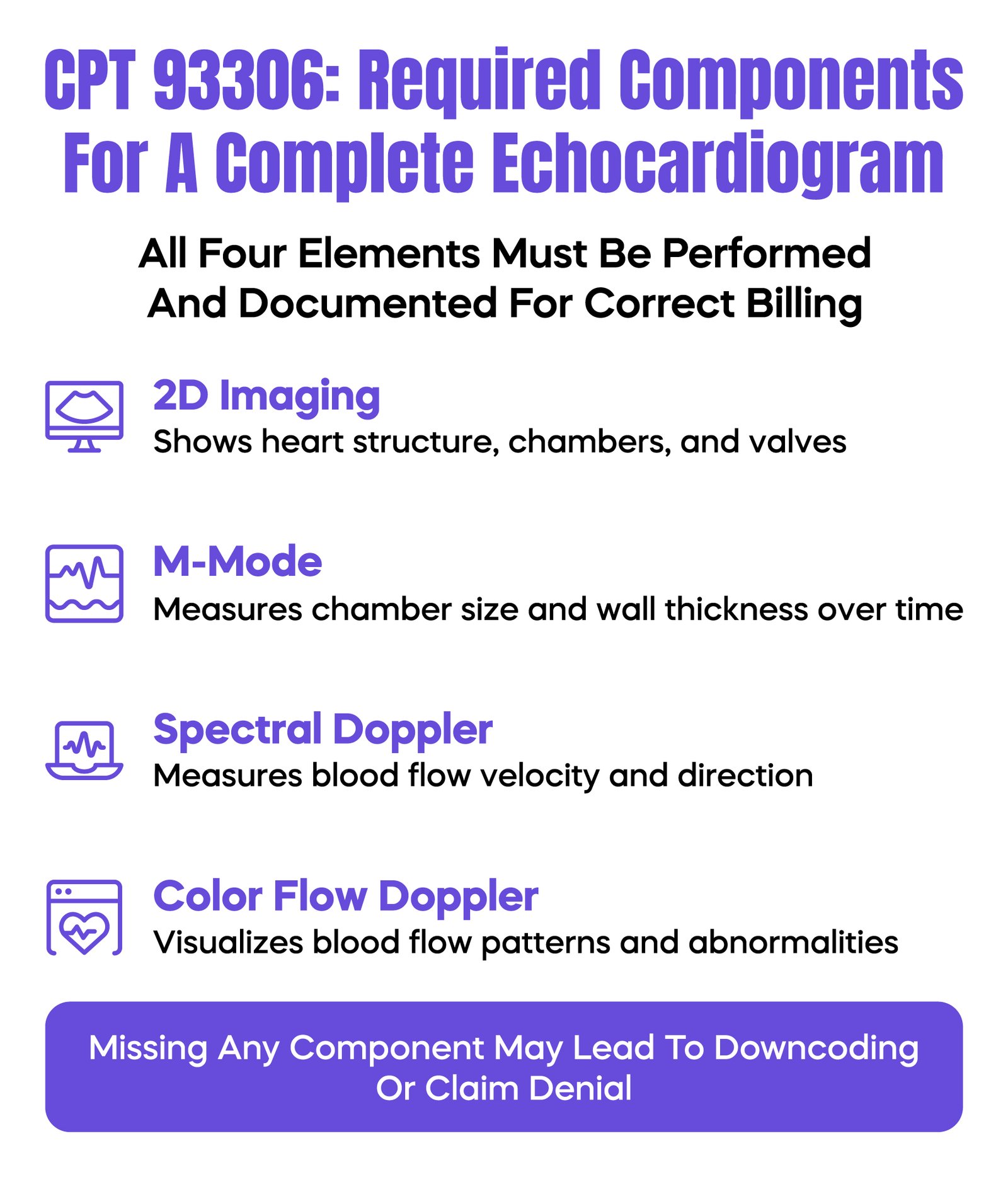
To bill CPT 93306 correctly, your report must support four required elements. Missing even one can lead to downcoding or denial.
First is 2D imaging, which provides a visual view of the heart chambers, valves, and walls.
Second is M-mode recording, which captures precise measurements of heart structures over time. This is often used to measure chamber size and wall thickness.
Third is spectral Doppler, which measures the speed and direction of blood flow. This helps assess valve function and detect abnormalities.
Fourth is color flow Doppler, which shows blood movement in color to identify abnormal flow patterns.
A common audit issue is the “incomplete echo” problem. The physician performs all components, but the report does not clearly mention one of them. The payer then treats the study as incomplete.
Two-dimensional imaging is the foundation of the study. It allows visualization of the heart’s structure and movement.
M-mode adds measurement precision. It tracks motion over time and is used to document chamber dimensions and wall thickness.
In a complete report, the physician should clearly describe:
If a report fails to mention key structures, it may appear incomplete to a payer. Even if the study was done correctly, missing documentation can still lead to denial.
Doppler is what separates CPT 93306 from lower-level echo codes.
Spectral Doppler provides measurable data about blood flow velocity. This is critical for diagnosing valve stenosis or regurgitation.
Color flow Doppler gives a visual map of blood movement. It helps detect abnormal or turbulent flow patterns.
A major audit risk occurs when Doppler is documented in text but not supported by stored waveforms or images. Many payers request proof during audits. If the data is not available, the payment may be recouped.
Another common issue is “template overdocumentation.” Some EHR systems automatically include Doppler findings even when not performed. This creates serious compliance risk.
CPT 93306 should only be used when a full echocardiographic study is medically necessary and performed.
It is appropriate for conditions such as heart failure, valve disease, cardiomyopathy, or unexplained cardiac symptoms.
However, it should not be used for limited evaluations. For example, checking only pericardial fluid or a single issue does not justify a complete study.
A common mistake in busy practices is billing CPT 93306 for every echo. Payers track utilization patterns. If a practice rarely bills for limited studies, it can trigger audits.
Another risk is repeat testing without clinical change. If there is no new symptom or condition, Medicare may deny the claim for lack of medical necessity.
Correct code selection is critical for both compliance and revenue.
CPT 93306 represents a complete study with all Doppler components.
CPT 93307 represents a complete study without full Doppler requirements. This is less common in modern practice.
CPT 93308 represents a limited or follow-up study focused on a specific clinical question.
For example, if a physician is only monitoring a known pericardial effusion, CPT 93308 is appropriate. Billing CPT 93306 in this case would be considered upcoding.
A comparison table should be added in the final layout to clearly show differences in scope, components, and reimbursement.
CPT 93306 can be billed as a global service or split into components.
Global billing includes both the technical and professional parts. The technical part covers equipment and staff. The professional part covers physician interpretation.
If only interpretation is billed, modifier 26 is required. If only the technical component is billed, modifier TC is used.
Claims are submitted using the CMS-1500 form. Errors such as incorrect place of service or missing modifiers can cause immediate rejection.
Clearinghouses often flag issues before submission. These edits should not be ignored. They are an early warning system for billing problems.
Practices must also follow payer-specific rules. Some insurers require stricter documentation or limit repeat studies.
Modifier accuracy directly affects payment.
Modifier 26 is used when the physician only interprets the study. Modifier TC is used for the technical portion.
A common real-world issue occurs in hospital settings. The hospital bills the technical component, and the physician bills the professional component. If both bill globally, one claim will be denied.
Another frequent mistake is missing modifiers. This can lead to duplicate billing denials or payment delays.
Correct modifier use ensures that each provider is paid correctly without conflicts.
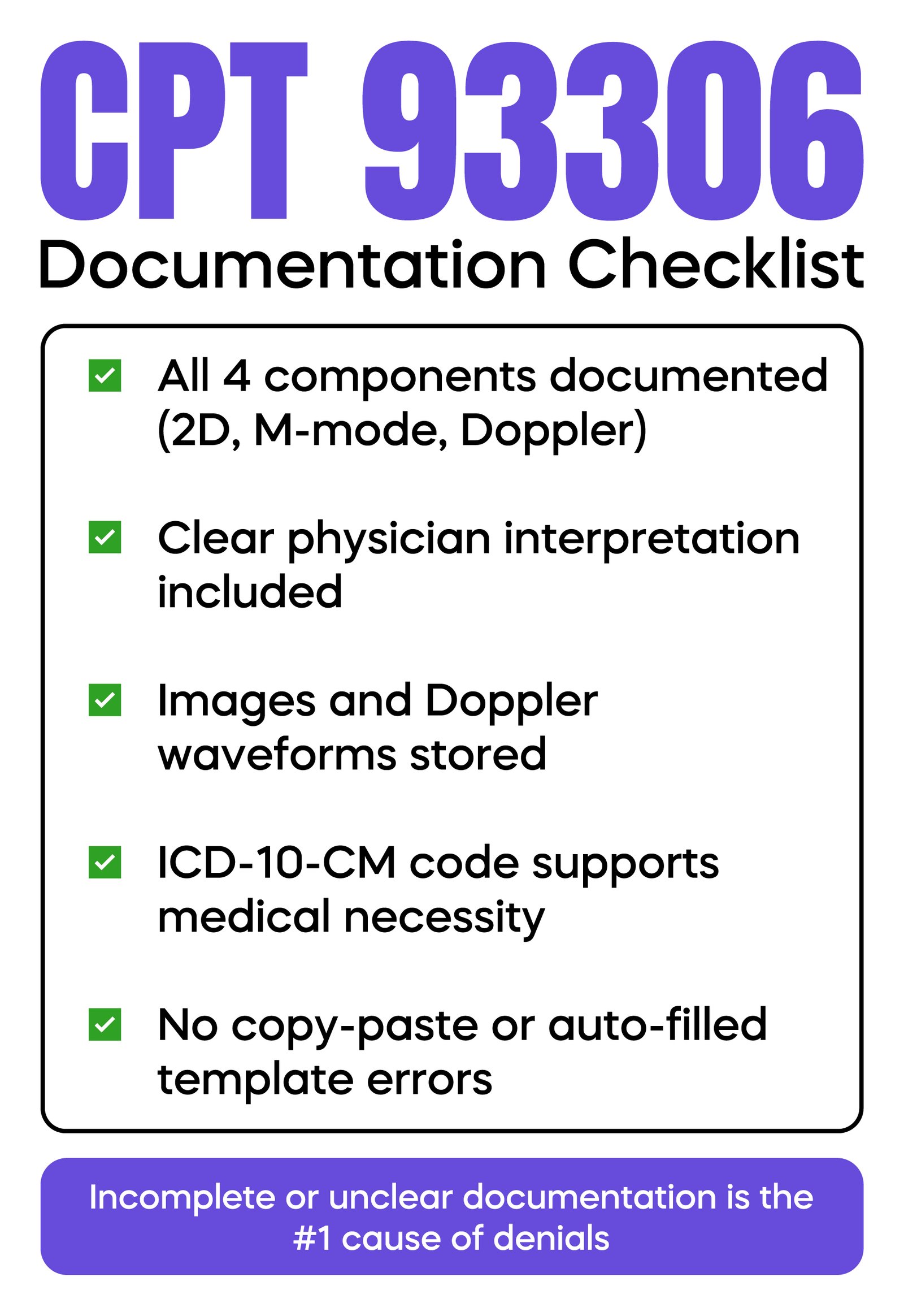
Documentation must clearly support both the procedure and the reason for it.
The report should include all four required components of the study. It must also include a clear interpretation, not just measurements.
Medical necessity must be supported by ICD-10-CM diagnosis codes. Common examples include chest pain, shortness of breath, heart murmurs, and heart failure.
Screening without symptoms is usually not covered. This is a common reason for denial.
Medicare Administrative Contractors use Local Coverage Determinations to review claims. If the diagnosis does not meet these guidelines, the claim will be rejected.
Reports should avoid copy-paste templates. Each report should reflect the individual patient’s condition.
CPT 93306 Reimbursement and Medicare Payment Insights
CPT 93306 generally has higher reimbursement than limited echo codes because it represents a complete study.
Payment depends on location, facility type, and whether the service is billed globally or by component.
Medicare uses the Physician Fee Schedule and relative value units to determine payment.
However, incorrect documentation can reduce payment through downcoding. This is one of the most common sources of hidden revenue loss.
Regular review of reimbursement trends can help practices identify issues early.
Most denials are preventable with proper processes.
A common denial occurs when Doppler or M-mode is not documented clearly. The claim is then reduced to a lower code.
Another issue is the lack of medical necessity. If the diagnosis does not justify the test, the payer will reject the claim.
Duplicate billing and modifier errors also lead to denials.
One overlooked issue is missing image storage. During audits, payers may request actual echo images. If they are not available, payment may be taken back.
Preventing denials requires alignment between clinical work, documentation, and coding.
CPT 93306 is a high-risk code from an audit perspective.
Auditors often look for patterns such as overuse of complete studies or repeated testing without clinical change.
They also check whether all required components are documented and supported by stored images.
A known risk is the “phantom Doppler” issue, where templates include Doppler findings that were not actually performed. This can lead to serious penalties.
Internal audits and regular documentation reviews can help reduce risk.
Improving CPT 93306 billing requires consistent habits.
Physicians should ensure every report clearly reflects a complete study. Coders should verify that documentation supports the selected code.
Billing teams should review modifiers and payer rules before submission.
Templates should be reviewed regularly to prevent overdocumentation errors.
Even small improvements in accuracy can significantly reduce denials and improve revenue.
CPT 93306 is both a high-value and high-risk code. Most billing problems come from small documentation gaps, incorrect coding, or modifier errors.
By ensuring complete documentation, accurate code selection, and proper modifier use, physicians can reduce denials and protect their revenue.
Consistency, clarity, and compliance are the key factors for long-term success in echocardiography billing.
Arj Fatima is a senior medical billing and coding specialist with deep expertise in U.S. cardiology billing, CMS compliance, and revenue cycle management. She helps physician practices reduce denials, improve documentation, and stay audit-ready through practical, experience-based guidance.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

