Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Physicians rarely think twice about giving an injection. It is routine, quick, and clinically straightforward. Yet from a billing standpoint, CPT 96372 is one of the most common sources of denials, underpayments, and audit exposure in U.S. medical practices. The issue is not complexity. It is inconsistent. Small gaps in documentation, incorrect modifier use, or missing drug codes can quietly reduce revenue over time.
Many practices lose legitimate income not because they do the work incorrectly, but because they fail to capture and report that work in a way that payers accept. This guide explains CPT 96372 in simple terms while addressing real billing risks, payer behavior, and compliance expectations so your practice can protect both revenue and audit readiness.
CPT 96372 is defined by the American Medical Association as the administration of a therapeutic, prophylactic, or diagnostic injection delivered either intramuscularly or subcutaneously. In plain terms, it represents the work involved in giving a shot.
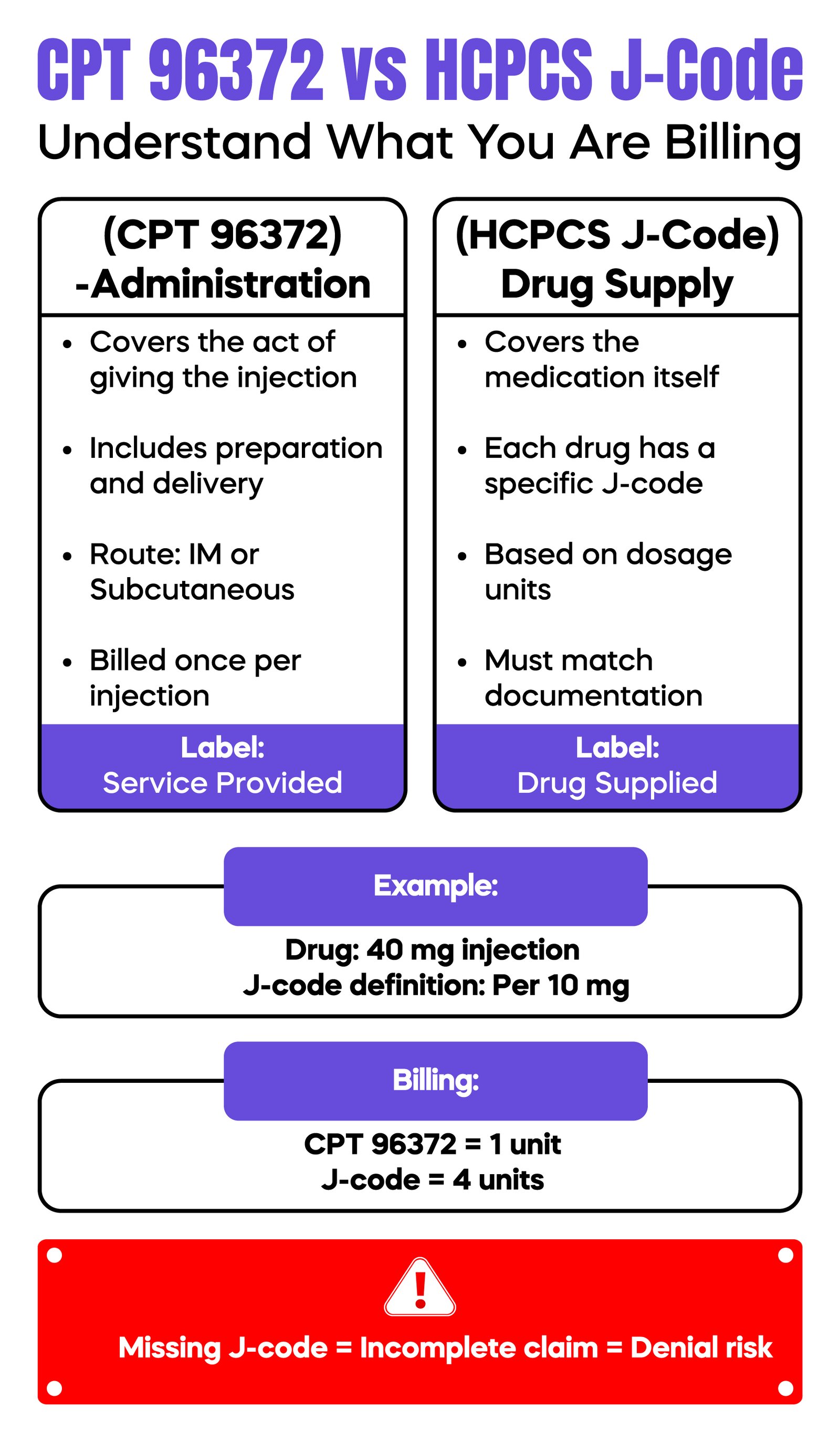
This distinction is critical. CPT 96372 does not cover the medication itself. It only covers the administration. The drug must be billed separately using HCPCS Level II codes defined by the Centers for Medicare and Medicaid Services.
For example, if a patient receives a steroid injection, the claim must include both the administration code and the appropriate J-code for the drug. When one of these elements is missing, the claim becomes incomplete. This is one of the most frequent and avoidable billing errors seen in outpatient practices.
CPT 96372 applies to injections that are therapeutic, preventive, or diagnostic in nature and are administered under the skin or into muscle tissue. These are typically performed in outpatient settings such as primary care clinics, urgent care centers, and specialty offices.
Common clinical uses include antibiotic injections, hormone therapy such as testosterone, vitamin B12 injections, and anti-inflammatory medications. The key requirement is that the injection must be medically necessary and appropriately documented.
It is equally important to understand when not to use this code. CPT 96372 should not be used for vaccines, as immunization administration has its own coding structure. It is also not appropriate for intravenous infusions or chemotherapy services, which fall under a different section of the CPT manual due to their complexity and monitoring requirements.
Misidentifying the type of injection is a simple error, but it leads to immediate claim rejection. Many denials occur because staff select 96372 out of habit without verifying the clinical context.
A major source of confusion in medical billing is the separation between administering a drug and supplying it. CPT 96372 represents the clinical effort of preparing and delivering the injection. The medication itself must be billed separately using an HCPCS J-code.
These drug codes are required on the CMS-1500 claim form and must align with the documentation in the medical record. Each J-code represents a specific drug and is often tied to unit-based billing. For instance, if a drug is defined as “per 10 mg” and a patient receives 40 mg, the claim must reflect four units.
Problems arise when the administration code is billed without a corresponding drug code, or when the units do not match the documented dosage. In some cases, claims are rejected before reaching the payer due to formatting errors, especially when National Drug Code information is missing or incorrect.
Another common issue involves mixing medications. If two drugs are combined into a single syringe and administered as one injection, only one unit of CPT 96372 can be billed, even though multiple J-codes may be reported. This distinction is often misunderstood and leads to overbilling risks.
Strong documentation is the foundation of correct billing. Payers do not reimburse based on what was done. They reimburse based on what is documented clearly and completely.
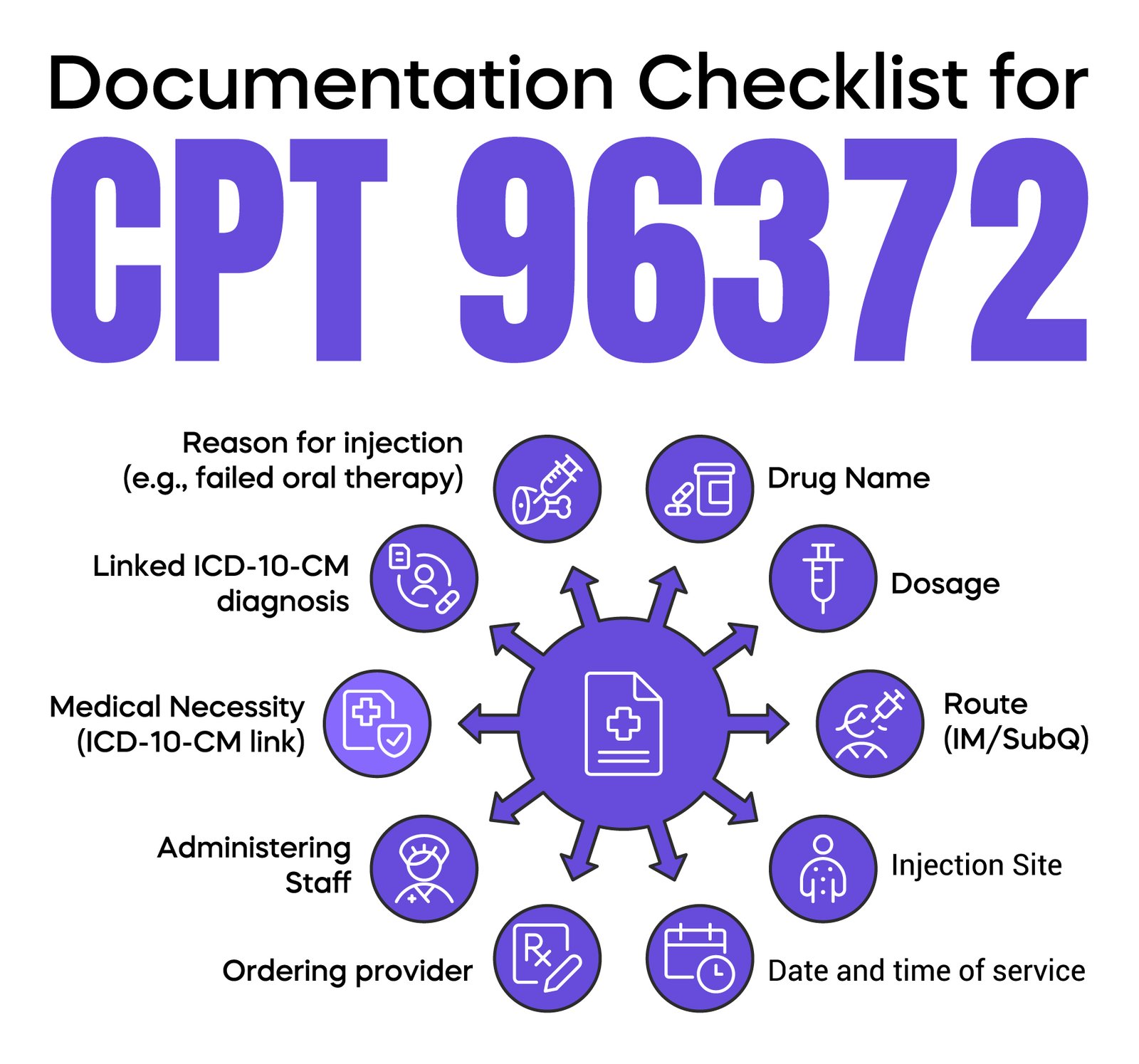
A proper injection note must include the medication name, dosage, route of administration, and exact injection site. It should also identify who ordered the injection and who administered it. The timing of the procedure and the patient’s response should be recorded as well.
However, the most important element is medical necessity. The documentation must explain why the injection was required. This could include failure of oral medications, need for faster therapeutic effect, or patient-specific limitations such as difficulty swallowing.
Generic statements such as “injection given” are not sufficient. Payers expect a clear clinical rationale supported by diagnosis coding using ICD-10-CM.
Electronic Health Records can create hidden risk. Many systems allow providers to copy forward previous notes. When identical documentation appears across multiple visits, especially for recurring injections, it raises red flags during audits. Each visit should reflect the patient’s current condition, even if the treatment plan remains consistent.
CPT 96372 can be billed with an Evaluation and Management service, but only when the visit involves significant and separate work beyond the injection itself. This distinction is critical for compliance.
Modifier 25 is used to indicate that the office visit is distinct from the injection service. It is applied to the E/M code, not the injection code. The documentation must clearly support two separate components: the medical decision-making associated with the visit and the procedural work of administering the injection.
For example, if a patient presents with worsening joint pain, and the physician performs a full evaluation, adjusts medications, and then administers an injection, both services can be billed. In contrast, if a patient visits solely for a scheduled injection with no additional evaluation, billing an E/M code would be inappropriate.
Overuse of modifier 25 is closely monitored by payers and Centers for Medicare and Medicaid Services contractors. Patterns of repeated use without strong documentation often trigger audits and payment recoupment.
Modifiers are often misunderstood and misused in injection billing. While they can help clarify services, they also increase scrutiny when applied incorrectly.
Modifier 25 is appropriate only when there is a clearly documented, separate evaluation service. If the documentation does not support additional physician work, the E/M portion of the claim will be denied.
Modifier 59 and its related X-modifiers may be used in limited situations when multiple injections are performed and must be identified as distinct services. However, these modifiers should not be used simply to override bundling edits. Doing so can raise compliance concerns and increase audit risk.
The safest approach is to ensure that the medical record itself clearly distinguishes each service. When documentation is strong, reliance on modifiers becomes minimal and defensible.
Medicare policies are established by the Centers for Medicare and Medicaid Services, but implementation is handled by Medicare Administrative Contractors through Local Coverage Determinations. These policies define when injections are considered medically necessary and how frequently they can be billed.
Commercial payers often follow Medicare guidelines but may introduce additional requirements such as prior authorization or stricter bundling rules. This creates variation that practices must manage carefully.
For example, some payers may limit the number of injections allowed per visit or require specific diagnosis codes to support coverage. Others may deny claims if frequency thresholds are exceeded without a strong justification.
Ignoring payer-specific policies is a common reason for denials, even when CPT coding is technically correct.
Reimbursement for CPT 96372 is relatively modest, but the volume of injections performed in most practices makes it financially significant. Payment rates vary based on geographic location, payer contracts, and the Medicare Physician Fee Schedule.
In most cases, Medicare reimbursement falls within a predictable range, but the total value of the service depends heavily on correct drug billing and accurate unit reporting.
Many practices focus only on the administration code and overlook errors in J-code billing. This leads to underpayment that is often unnoticed. Over time, these small losses accumulate and impact overall revenue cycle performance.
Denials for CPT 96372 tend to follow consistent patterns. Understanding these patterns allows practices to correct issues before they affect cash flow.
One of the most common problems occurs when an office visit is billed without the proper use of modifier 25. In these cases, the payer assumes the visit was only for the injection and denies the E/M service. The opposite problem also occurs when modifier 25 is used without sufficient documentation, leading to the same outcome.
Missing or incorrect HCPCS drug codes create another major issue since the injection code represents only the administration; failure to include the drug results in incomplete billing.
Medical necessity is also a frequent trigger. If the diagnosis does not justify the injection, the claim is denied regardless of procedural accuracy. This is especially common in recurring therapies, where documentation does not reflect changes in the patient's condition.
Duplicate billing and a lack of clarity in multiple injection scenarios further increase the risk. When multiple injections are performed, each must be supported by documentation that clearly identifies separate sites or clinical purposes.
A common audit scenario involves repeated injections with identical documentation across visits. This pattern suggests a lack of individualized care and often results in recoupment of payments.
| Denial Reason | Root Cause | Fix |
| Missing J-code | Incomplete claim | Add HCPCS code |
| E/M denied | Wrong modifier 25 | Fix documentation |
| Medical necessity | Weak ICD-10 | Improve diagnosis |
| Duplicate billing | Poor clarity | Document distinct injections |
Injection services are considered high-risk from an audit perspective because they are easy to perform and easy to overbill. Payers and Medicare contractors monitor patterns closely.
Red flags include unusually high frequency of injections, repeated use of modifier 25, and consistent use of the same diagnosis without variation. Lack of detail in procedure notes or reliance on copied documentation also increases audit exposure.
National and local coverage policies define when injections are appropriate. Failure to align documentation with these policies creates compliance risk even if services are clinically justified.
Practices that perform regular internal audits and train staff on documentation standards are better positioned to avoid these issues. Denial trends should be tracked and reviewed to identify patterns before they escalate into larger financial problems.
CPT 96372 is used to bill the administration of therapeutic, prophylactic, or diagnostic injections given intramuscularly or subcutaneously. It does not include the medication, which must be billed separately using HCPCS J-codes. Proper documentation, correct modifier use, and adherence to payer-specific rules are essential to avoid denials and audits.
Arj Fatima is a senior medical billing specialist with hands-on experience in U.S. healthcare reimbursement systems. She works closely with physicians and practice owners to reduce claim denials, improve documentation accuracy, and maintain compliance with CMS guidelines. Her expertise includes CPT coding, modifier usage, audit prevention, and revenue cycle optimization across multiple specialties.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

