Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Interventional cardiology claims are high-value and high-risk. One small coding error can trigger bundling denials, modifier rejections, or post-payment audits. Many cardiologists perform balloon angioplasty correctly from a clinical standpoint, yet revenue is delayed or reduced because CPT Code 92920 was reported incorrectly.
This guide explains CPT Code 92920 from a strict U.S. billing and compliance perspective. It reflects current guidance from the American Medical Association CPT manual and payment logic used by the Centers for Medicare & Medicaid Services. The goal is simple. Protect your revenue. Reduce audit risk. Ensure defensible documentation.
CPT Code 92920 describes percutaneous transluminal coronary angioplasty (PTCA) performed in a single major coronary artery or its branches. In plain language, this means you use a catheter and balloon to dilate a narrowed coronary artery. No stent is placed. No atherectomy is performed.
The code includes all angioplasty work within one major coronary artery territory and its associated branches. If you dilate the Left Anterior Descending artery and also treat a diagonal branch in the same session, you report 92920 once for that LAD family.
This is territory-based reporting, not branch-based reporting.
Interventional cardiology follows a strict hierarchy. More complex procedures include less complex ones performed in the same vessel.
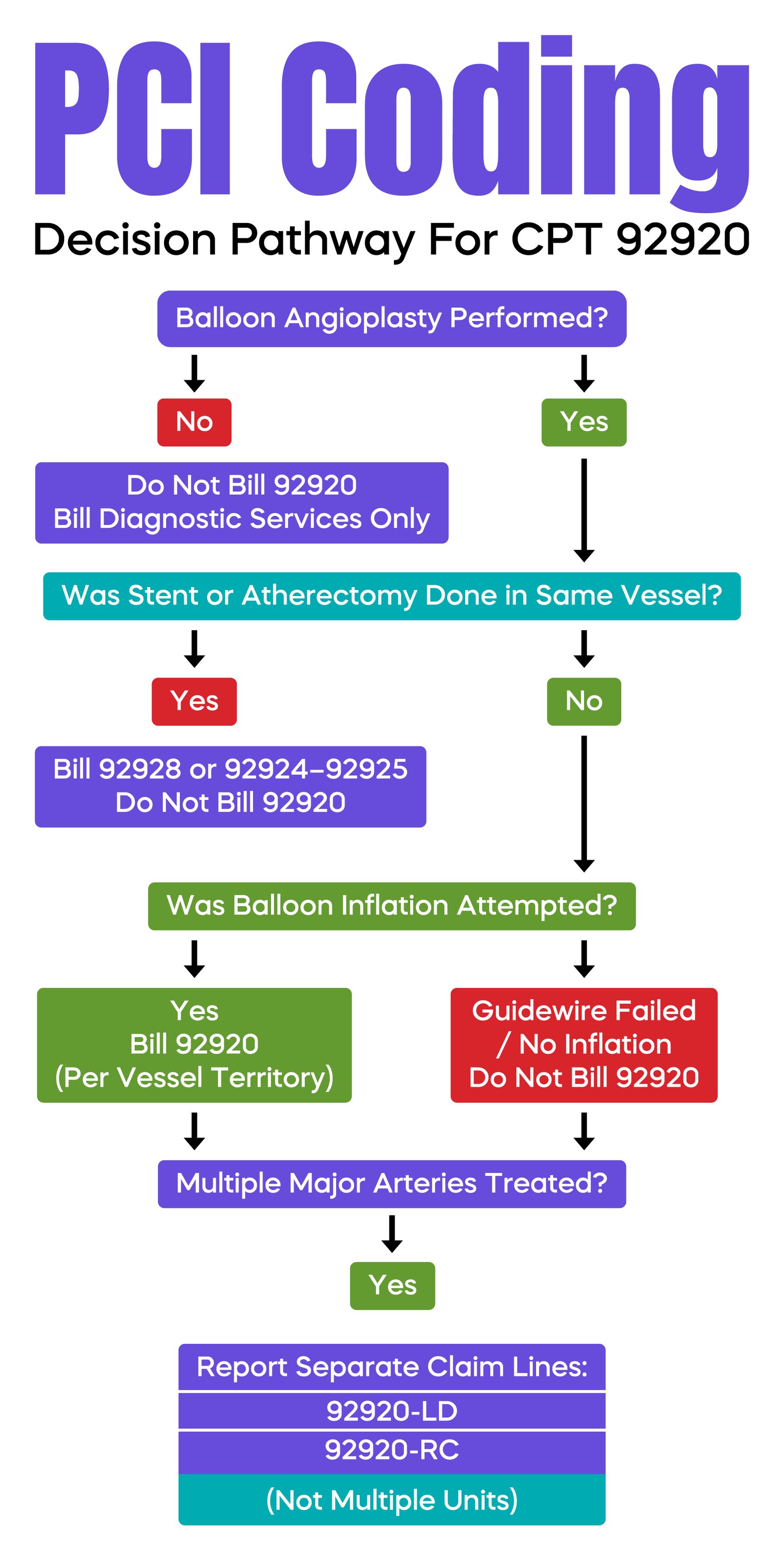
CPT 92920 represents balloon angioplasty alone. If a stent is placed in the same artery during the same session, CPT 92928 must be reported instead. The angioplasty performed before stent deployment is included in 92928 and cannot be reported separately.
Attempting to bill both 92920 and 92928 in the same vessel is considered unbundling. Under CMS National Correct Coding Initiative edits, the lower-level service will be denied.
The key rule is this. Report CPT 92920 only when angioplasty is the highest level of intervention performed in that specific artery during that encounter.
CPT 92920 is reported once per major coronary artery territory.
The main territories include:
If angioplasty is performed only in two separate major vessels, the code must be reported on separate claim lines with different anatomical modifiers. It should not be billed as multiple units on one line.
Correct reporting example:
92920-LD
92920-RC
Medicare systems process these as distinct anatomical services, not quantity-based units. Reporting two units on a single line can cause processing errors.
If multiple branches within the same vessel family are treated, you still report only one unit for that territory.
Anatomical modifiers tell the payer which artery was treated. Without them, the claim may be denied or suspended.
Common modifiers include:
LD – Left Anterior Descending
LC – Left Circumflex
RC – Right Coronary
LM – Left Main
RI – Ramus Intermedius
Each treated artery must be listed on a separate claim line with the appropriate modifier. This ensures accurate adjudication and reduces duplicate-service denials.
Diagnostic catheterization codes 93454 through 93461 may be separately billable when strict criteria are met.
To bill both diagnostic angiography and CPT 92920 in the same session, documentation must clearly show that the decision to intervene was made based on new diagnostic findings obtained during that encounter.
If prior angiographic data were already available and the intervention was planned, the diagnostic portion is generally considered bundled.
When criteria for separate reporting are met, a modifier such as 59 or XS may be required to indicate a distinct procedural service.
Important clarification. Radiological supervision and interpretation are bundled into CPT 92920 only for the interventional component. Separately reportable diagnostic angiography retains its own supervision and interpretation component when properly supported.
Medical necessity is not determined by stenosis percentage alone.
While clinical practice often references numerical thresholds, CMS does not mandate a fixed percentage in a National Coverage Determination. Medical necessity must be supported by symptoms, ischemia, hemodynamic significance, or objective testing such as fractional flow reserve.
Your documentation must clearly connect:
ICD-10-CM codes must accurately reflect the treated condition and coronary territory. Generic coronary artery disease codes without a documented clinical context may trigger automated medical necessity denials.
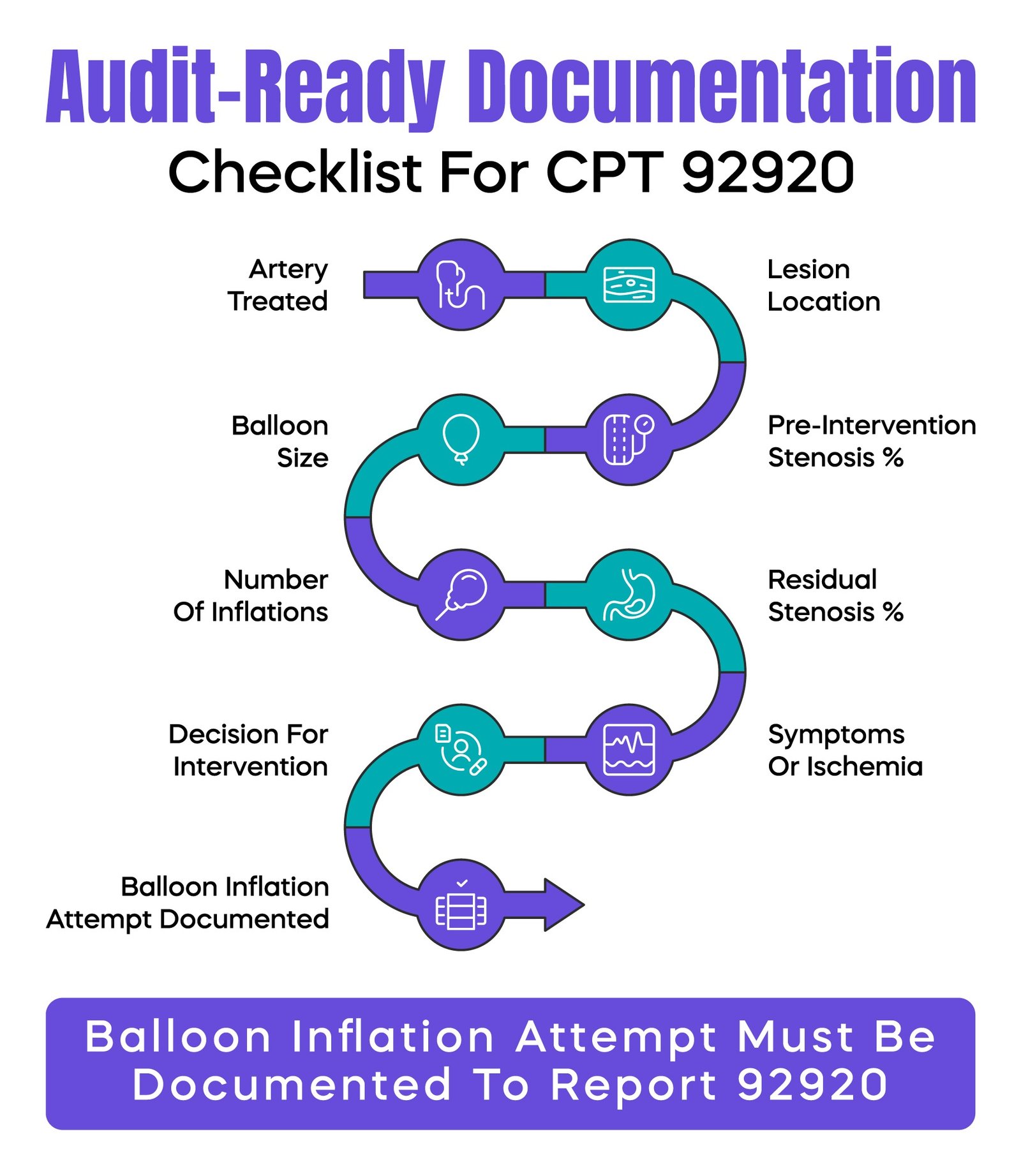
The operative report must be precise and structured.
Include:
If angioplasty is attempted but not fully successful, CPT 92920 may still be reported, provided balloon inflation was attempted and documented.
However, if the guidewire cannot cross the lesion and no balloon inflation is attempted, CPT 92920 is not reportable. Only the services actually performed may be billed.
This distinction is frequently reviewed during audits.
Reimbursement for CPT 92920 includes a professional component and a technical component.
The professional component reflects physician work, judgment, and skill. The technical component reflects facility resources and equipment.
Radiological supervision related to the intervention is packaged into the primary code. Accurate documentation ensures appropriate capture of physician work relative value units.
Certain services may be separately reportable when medically necessary and documented.
Examples include intravascular ultrasound and fractional flow reserve. These have distinct CPT codes and are not automatically included in 92920.
However, they must be clearly justified in the medical record. Routine or unsupported reporting increases audit exposure.
The most common denial is bundling with a higher-level intervention, such as stent placement or atherectomy in the same vessel.
Other frequent denials include:
Preventive strategies include standardized operative templates, coder-physician communication, and internal chart audits focused on vessel identification and hierarchy compliance.
A patient presents with unstable angina. Diagnostic angiography reveals a new 85 percent proximal RCA lesion not previously documented. Based on these findings, balloon angioplasty is performed without stent placement.
The record documents ischemic symptoms, lesion severity, balloon details, and residual stenosis. In this case, the diagnostic catheterization may be separately reported if criteria are met, and CPT 92920-RC is billed for the angioplasty.
A patient with known multivessel disease undergoes intervention. Balloon angioplasty is performed in the LAD, followed by stent placement in that same artery.
Only CPT 92928-LD is reported. The angioplasty is included. Reporting 92920 separately would be noncompliant.
A complex lesion is approached in the LCX. The guidewire successfully crosses the lesion. Balloon inflation is attempted, but full dilation is not achieved due to calcification. The attempt is clearly documented.
CPT 92920-LC may be reported because balloon dilation was attempted.
If the guidewire had failed to cross and no balloon was inflated, 92920 would not be appropriate.
Percutaneous coronary intervention services are high-dollar procedures. They are frequently reviewed under payer audit programs.
Compliance depends on:
Periodic internal audits can identify patterns of incorrect bundling or modifier errors before external reviewers do.
CPT Code 92920 appears straightforward, but errors in hierarchy, modifiers, and documentation create significant revenue and compliance risk. Accurate territory-based reporting, separate claim lines per artery, proper documentation of balloon attempt, and clear medical necessity support are essential.
In interventional cardiology billing, precision protects both reimbursement and audit defensibility.
Arj Fatima is a senior medical billing strategist with over 10 years of experience in U.S. interventional cardiology revenue cycle management. She has worked with hospital-based cardiac programs and independent cardiology groups to reduce PCI denials, correct modifier misuse, and strengthen compliance under federal and commercial payer policies. Her focus is defensible documentation, accurate CPT reporting, and long-term revenue protection for physicians.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

