Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Every doctor knows that a complex patient visit involves more than just the time spent in the exam room. It involves the mental weight of managing a patient’s long-term health, tracking their chronic conditions over the years, and being the single point of trust for their medical journey. For a long time, the standard office visit codes did not pay for this extra cognitive effort. Medicare created HCPCS code G2211 to fix this gap. This code is an add-on payment that rewards you for the "longitudinal" care you provide. In simple terms, it pays you for being the doctor who knows the patient best. Using this code correctly according to current Medicare standards can significantly increase your practice revenue while accurately reflecting the work you already do.
The healthcare system is moving away from paying only for procedures and toward paying for the relationship between a doctor and a patient. HCPCS code G2211 is a "complexity" code. It is not about how sick the patient is on a single day. Instead, it is about your commitment to managing that patient’s total care over time. When you see a patient for a cold, but you are also the person managing their diabetes, heart failure, and mental health, your work is more complex than a quick urgent care visit. Medicare acknowledges that this type of care requires more documentation, more follow-up, and more expertise. By adding G2211 to your claim, you are telling the payer that you are the primary coordinator for this patient’s serious or ongoing health journey.
The most important term to learn for G2211 is the "longitudinal relationship." This is a professional way of saying you plan to see this patient for a long time. You are the "medical home" for their specific problem or their general health. Under current billing rules, this relationship is clearly defined. You do not need to have seen the patient for ten years to bill this code. You can bill it during a first visit if your medical record shows that you intend to be the primary manager of their condition moving forward. This relationship exists when you are the one responsible for the "continuous" care of the patient. If you are a specialist managing a single complex condition like Crohn’s disease or Lupus, you also have a longitudinal relationship. You are the expert who will guide them through that specific chronic journey for the foreseeable future.
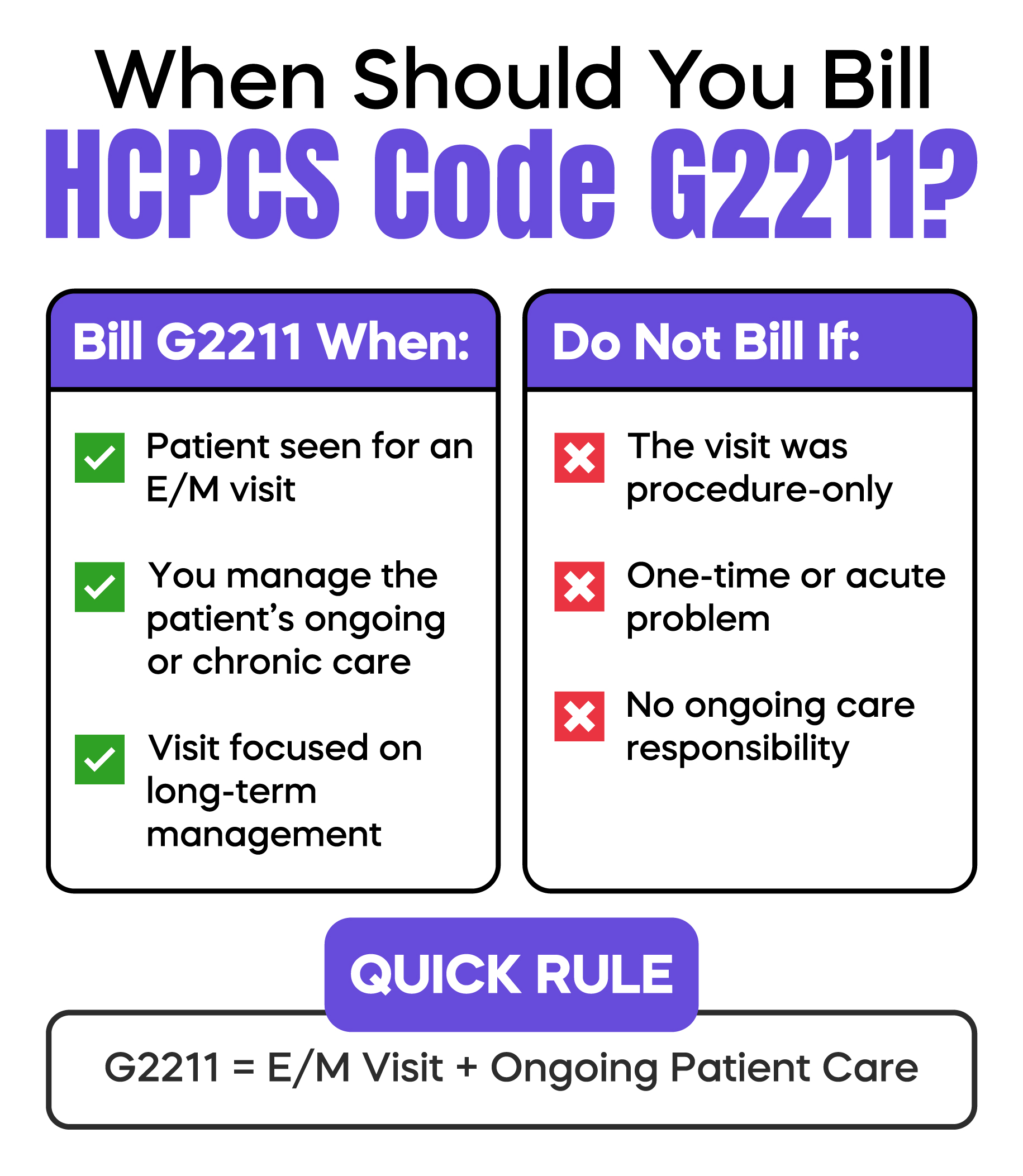
To get paid for G2211, you must follow specific billing rules. First, G2211 is an add-on code. You cannot bill it by itself. It must be paired with a primary Evaluation and Management (E/M) code. While this originally applied mostly to office visits, the scope has grown significantly to support longitudinal care in other settings. If the primary code is denied, the G2211 add-on will also be denied. Most importantly, you should not use this code if the visit is purely for a simple, one-time problem where you do not plan to see the patient again, such as a simple mole removal or a basic flu shot for a person who has a different primary doctor.
A major standard in modern billing is the inclusion of diverse care settings for G2211. While the code was initially limited to office visits, current Medicare policy allows it for doctors providing long-term care in the patient’s home or a facility. This includes Home/Residence E/M codes 99341 through 99350. Furthermore, practitioners in post-acute settings can now utilize G2211 with Nursing Facility care codes 99304 through 99310 and NF discharge management codes 99315 and 99316. This expansion ensures that geriatricians and house-call clinicians are compensated for the "invisible work" of coordinating complex care for homebound or institutionalized populations.
Reporting G2211 with Modifier 25 is one of the most misunderstood areas of Medicare policy. Modifier 25 identifies a significant, separately identifiable E/M service on the same day as a procedure. Contrary to popular belief, Medicare does not automatically prohibit billing G2211 when Modifier 25 is present. You may report G2211 on the same date as a procedure if the E/M visit represents the ongoing management of a serious or complex condition and is medically necessary beyond the procedure itself.
However, CMS applies strict scrutiny here. You should only bill the add-on when the visit is not "primarily" for the procedure. For example, if a patient visits for their chronic heart failure management and you happen to perform a minor skin biopsy, G2211 is applicable if your documentation shows the complexity of the heart failure management was the driving force of the encounter. Conversely, if the visit was scheduled solely for the biopsy and you only briefly check their medications, G2211 would likely be denied.
Documentation is your best defense against an audit. For G2211, you do not need to write a long narrative. You do need to prove two things in your note. First, you must show the "why." Why is this visit complex? Is it because you are balancing multiple medications? Is it because the patient has social struggles that make following a plan difficult? Second, you must show the "future." Your note should clearly state that you are managing this patient for the long term. A simple sentence like "I will continue to manage this patient's chronic hypertension and monitor for long-term complications" is very helpful. This confirms the longitudinal nature of the visit.
Many EHR systems allow you to click a box that drops a standard paragraph into every note. Auditors flag this as "cloning," which can lead to payment clawbacks. Instead, make your note specific to the patient’s longitudinal plan. Additionally, be wary of billing G2211 for visits that only address acute, self-limited problems without a tie-back to the longitudinal relationship. If a patient you’ve never seen before comes in for a simple viral cough and you don't document a plan for ongoing management of a complex condition, G2211 is not appropriate. Your notes must illustrate your responsibility for the patient's "consistency and continuity" of care.
The payment for G2211 typically averages around 16 dollars per visit nationally. While this may seem small, the cumulative impact is substantial. For a practitioner seeing 20 patients a day and applying this code to 75% of those visits, the annual revenue increase can range between 50,000 and 60,000 dollars. This reimbursement accounts for the cognitive load, the time spent reviewing cumulative history, coordinating with specialists, and updating complex care plans outside of the face-to-face encounter. It is important to note that while G2211 has no assigned global period, Medicare may still deny it if the E/M service is deemed to be primarily peri-procedural care rather than the ongoing management of a complex condition.
HCPCS code G2211 is a complexity add-on code for E/M visits in office, home, and nursing facility settings. It compensates physicians for the cognitive effort of longitudinal patient care. It can be billed with Modifier 25 if the E/M service is medically necessary and addresses long-term management separate from the procedure.
Arj Fatima is a Senior Revenue Cycle Strategist with 15+ years of experience in U.S. medical billing. She specializes in Medicare policy, CPT/HCPCS coding, and protecting practices from audit risk through accurate documentation strategies.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

