Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us
As a chiropractic physician, your responsibility is clinical care. As a practice owner, your responsibility is financial stability. In today’s Medicare Part B and commercial payer environment, claim rejections are rarely random. They are signals of breakdowns inside your Revenue Cycle Management (RCM) system.
When rejections increase, Accounts Receivable (AR) stretches. Cash flow slows. Staff spend hours correcting preventable errors. If your rejection rate exceeds 5% or your AR consistently crosses 40 days, the issue is process, not patient volume.
Eliminating chiropractic claim rejections requires alignment with CMS regulations, MAC enforcement policies, documentation standards, and payer automation logic. This article outlines how to build that alignment.
Chiropractic billing under Medicare Part B is governed by the Centers for Medicare & Medicaid Services (CMS). The controlling policy is found in the Medicare Benefit Policy Manual, Chapter 15, Section 240. It states clearly that Medicare covers only manual manipulation of the spine to correct a subluxation.
This limitation is foundational. Medicare does not broadly cover chiropractic services. It covers a specific service under specific documentation rules.
Although CMS establishes national policy, claims are processed regionally by Medicare Administrative Contractors (MACs). Each MAC publishes Local Coverage Determinations (LCDs), which function as the practical rulebook for your state. These LCDs define medical necessity language, documentation expectations, and frequency parameters.
If your documentation does not align with your MAC’s LCD wording, your claim may be denied even when clinically appropriate.
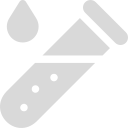
A rejection occurs before the claim is adjudicated. It fails validation during electronic 837P processing or CMS-1500 claim form checks. Rejections are typically technical errors, such as incorrect demographics, invalid diagnosis codes, or missing mandatory fields like the Initial Treatment Date in Box 14.
A denial occurs after the payer reviews the claim. The service was processed, but payment was refused. Common denial codes include:
Rejections delay revenue. Denials threaten compliance and increase audit exposure. Both must be managed, but they require different corrective strategies.
Medicare chiropractic billing depends on a precise relationship between procedure codes and subluxation diagnosis codes. The number of spinal regions treated must match the number of documented subluxation diagnoses.
| CPT Code | Regions Treated |
| 98940 | 1–2 regions |
| 98941 | 3–4 regions |
| 98942 | 5 regions |
| ICD-10 Code | Region |
| M99.01 | Cervical |
| M99.02 | Thoracic |
| M99.03 | Lumbar |
| M99.04 | Sacral |
| M99.05 | Pelvic |
A common rejection occurs when a provider bills 98941 for three regions but lists only two M99.0x codes. The payer’s system interprets this as insufficient proof of the number of regions treated. The result is an automatic rejection or medical necessity denial.
Each region adjusted must have a corresponding M99.0x diagnosis and must be properly linked on the claim.
Many rejections occur at the field level. The most common risk areas on the CMS-1500 claim form include the following:
| Box | Field | Why It Matters |
| 14 | Date of Current Illness | Mandatory for Medicare chiropractic claims |
| 21 | Diagnosis Codes | Must list correct M99.0x codes |
| 24D | Modifiers | AT is required for active care |
| 24E | Diagnosis Pointer | Must correctly link CPT to diagnosis |
| 24J | Rendering NPI | Must match enrollment records |
| 31 | Provider Signature | Must align with NPI |
Electronic 837P claims follow identical validation logic before they reach the MAC. Clearinghouse edits help, but they do not replace internal review processes.
Modifier misuse is one of the leading causes of chiropractic denials.
The AT modifier signals active, corrective treatment. Without it, Medicare assumes maintenance care and denies payment. However, the AT modifier must be supported by documentation demonstrating functional improvement and medical necessity under the P.A.R.T. criteria.
The GA modifier may be used when services are expected to be denied, and a valid Advance Beneficiary Notice (ABN) is signed before treatment. Without a properly executed ABN, GA use is non-compliant.
Modifier 25 applies only when a significant, separately identifiable Evaluation and Management (E/M) service is performed on the same day as spinal manipulation. Routine pre-adjustment assessment does not qualify. Overuse of Modifier 25 frequently triggers audits from both Medicare and commercial payers.
To establish medical necessity, documentation must include at least two of the following P.A.R.T. elements:
One of the documented findings must be Asymmetry or Range of Motion.
Prolonged use of the AT modifier without updated exams increases audit risk. Best practice is to conduct a formal re-exam every 30 days or 12 visits and document measurable improvement. If the patient plateaus, continuing to bill active treatment may be considered non-compliant.
Commercial insurers add complexity beyond Medicare rules. Many plans impose annual visit caps, preauthorization requirements, and functional outcome reporting.
For example, if a plan allows 20 visits annually and the 21st visit is not authorized, the claim will likely be denied for exceeding benefits. These denials are preventable through front-end eligibility verification and visit tracking.
Monitoring performance metrics is essential for controlling rejections.
| KPI | Target Benchmark | Purpose |
|---|---|---|
| Clean Claim Rate | 98% | Measures first-pass accuracy |
| Days in AR | Under 35 days | Indicates payment speed |
| Rejection Rate | Under 5% | Signals clerical efficiency |
| Net Collection Rate | 95%–105% | Reflects retained revenue |
Consistent review of these metrics allows early detection of workflow breakdowns.
Chiropractic claim rejections are not random administrative annoyances. They are measurable failures in system design. When coding aligns with CMS policy, documentation reflects LCD language, and internal reviews catch field-level errors before submission, revenue stabilizes.
In a healthcare environment increasingly driven by automation and audit scrutiny, billing precision is no longer optional. It is operational protection.
Clinical excellence builds patient trust. Documentation discipline protects your practice.
What does Medicare cover for chiropractors?
Only manual spinal manipulation to correct a subluxation under Medicare Part B.
Is an X-ray required to prove subluxation?
No. CMS allows proof by X-ray or physical exam using P.A.R.T. criteria.
Arj Fatima is a senior U.S. medical billing strategist specializing in chiropractic Revenue Cycle Management, CMS compliance, and audit defense. She works with solo practitioners and multi-provider groups to strengthen documentation standards, improve clean claim rates, and reduce denials under Medicare and commercial payer rules.
Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.