Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us


Many physicians hesitate before selecting CPT Code 99215. You may worry about triggering an audit. You may fear payer scrutiny from Medicare or commercial payers. Because of that fear, many physicians undercode and bill 99214 even when the visit involved complex decision making, unstable disease, or high-risk treatment adjustments.
Undercoding is not a compliance strategy. It reduces earned revenue and misrepresents the intensity of your cognitive work. CPT Code 99215 exists to capture true high-level outpatient management. When documentation reflects real complexity, it is appropriate and defensible.
This guide explains how to use CPT Code 99215 correctly under current Evaluation and Management rules, with precise documentation standards.
CPT Code 99215 is defined by the American Medical Association within the Current Procedural Terminology system. It applies to office or outpatient visits for established patients.
An established patient has received professional services from you or another physician of the same specialty in your group within the past three years.
Under the 2021 AMA CPT E/M guidelines adopted by CMS and most commercial payers, code selection is based on either:
History and physical exam must be medically appropriate, but they no longer determine the level of service.
CPT 99215 represents the highest level of established patient outpatient care. It reflects substantial cognitive effort, high clinical risk, or extended physician time.
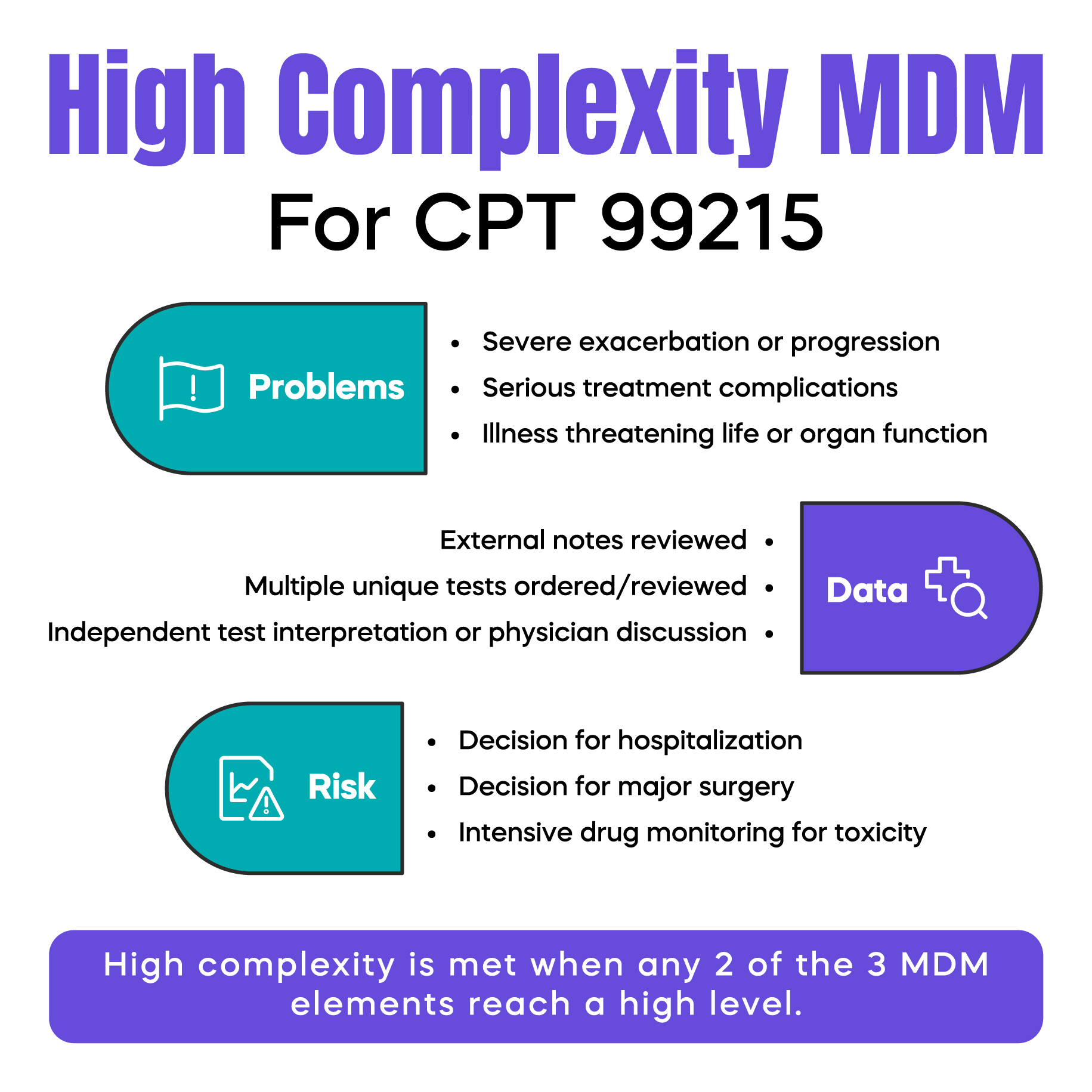
Medical Decision Making is the most common pathway to 99215. To qualify, documentation must meet two of the following three elements at a high level:
You do not need all three at the highest level. Two are sufficient.
The MDM framework measures the intensity of your thinking, risk assessment, and management decisions. It reflects clinical judgment, not checkbox documentation.
To meet high complexity in the problem category, you must address at least one of the following:
For example, a patient with heart failure who presents with worsening edema and shortness of breath requiring urgent diuretic adjustment may qualify.
Another example is uncontrolled diabetes with rising A1C, new neuropathy, and the need for insulin adjustment. However, uncontrolled diabetes alone does not automatically qualify. Documentation must show severe progression, treatment escalation, or threat to bodily function.
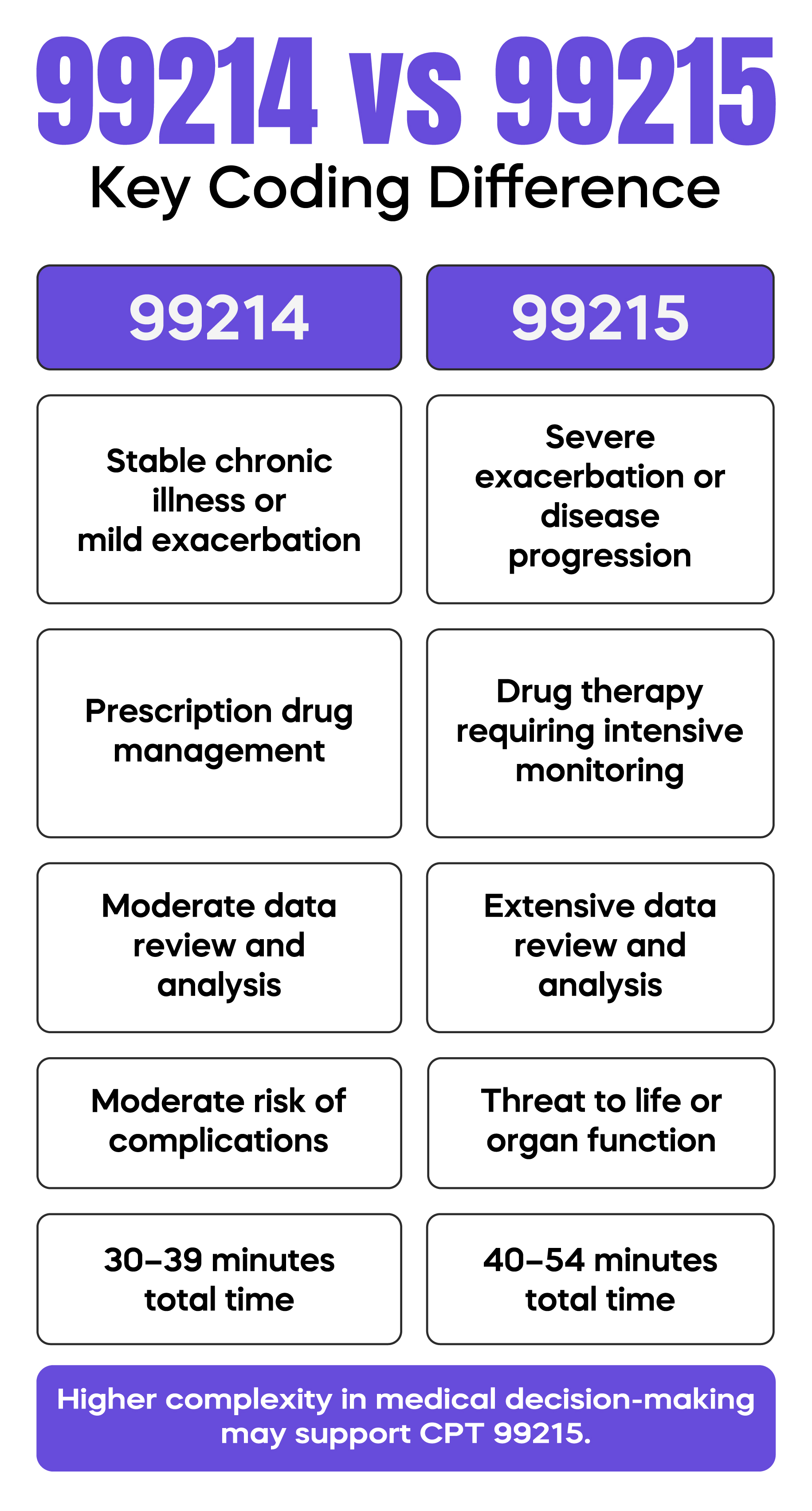
Multiple stable chronic conditions without change usually support 99214, not 99215.
The key question is whether the condition required intensive management or carried substantial risk during that encounter.
The second MDM element evaluates the work of gathering and analyzing data.
For 99215, this often requires extensive data activity across multiple categories. Examples include:
A unique source refers to a different physician, specialty, or healthcare facility.
Documentation must be specific. Writing “labs reviewed” is insufficient. Identify which labs, imaging, or consultation notes were reviewed and explain how they influenced management.
If you personally interpret an ECG tracing or imaging study and document your interpretation separately from the formal report, that supports higher data complexity.
The third MDM element evaluates risk.
For CPT 99215, the risk must be high. This does not require immediate collapse. It refers to management decisions involving significant potential harm or life-altering outcomes.
Examples of high risk include:
Prescription drug management alone typically supports moderate risk, which aligns with 99214. It reaches high risk only when intensive monitoring for toxicity is required or when management decisions carry significant potential for serious harm.
When documenting risk, explain why your management decision carries danger. Do not rely on the diagnosis alone. Auditors evaluate reasoning, not assumptions.
If MDM does not clearly support high complexity, CPT 99215 may be selected based on total time.
Under the 2021 AMA CPT E/M guidelines adopted by CMS and most commercial payers, 99215 requires 40 to 54 minutes of total physician or qualified healthcare professional time on the date of service.
Total time includes:
Only a physician or a qualified healthcare professional counts. Staff time does not count.
Best practice is to document exact minutes. For example: “Total time spent on date of service was 48 minutes.” Briefly summarize major activities performed during that time.
A common error is labeling a patient as “stable” while adjusting therapy due to subtle deterioration.
If you change treatment because the current plan is failing or the risk is increasing, the condition is not stable. That escalation may support 99215.
Always evaluate the reason behind management decisions. If your actions reflect high-level problem complexity or high risk, reassess whether 99215 is appropriate.
Medical necessity remains the controlling factor for all coding decisions.
Even when time thresholds are met, the service must be reasonable and necessary for that patient on that date.
The Centers for Medicare & Medicaid Services and commercial payers monitor E/M utilization patterns. Physicians with unusually high 99215 rates compared to specialty peers may be reviewed.
Common audit triggers include:
Specific, individualized documentation is your strongest audit defense.
If you obtain history from a caregiver because the patient cannot provide reliable information, document that clearly. An independent historian is a recognized data element that can support higher data complexity when appropriate.
When ordering imaging or advanced diagnostics, link each order to the diagnosis being evaluated. Explain how the result will influence your management plan.
This strengthens medical necessity and supports defensible coding.
Accurate 99215 coding affects more than a single claim. Chronic undercoding reduces long-term practice revenue and distorts workload reporting.
Claims are submitted electronically or via the CMS-1500 and require correct diagnosis linkage using ICD-10-CM codes.
If diagnosis codes do not reflect severity or complications, payers may downcode or deny the claim despite strong documentation.
Effective revenue cycle management requires alignment between documentation, coding level, and diagnosis specificity.
CPT 99215 may be billed for telehealth visits if the encounter meets MDM or time requirements.
However, payer policy, place-of-service coding, and modifier requirements still apply. Always verify current payer rules before submission.
CPT Code 99215 represents the highest level of established patient outpatient management. It reflects high medical decision-making or extended physician time. It is appropriate when documentation clearly demonstrates severe problem complexity, extensive data analysis, or high management risk.
Undercoding reduces revenue. Overcoding without support increases audit risk. The solution is precise, patient-specific documentation that explains your reasoning and supports medical necessity.
When used correctly, 99215 is both compliant and financially appropriate.
Arj Fatima is a senior medical billing strategist with over 10 years of experience in U.S. healthcare reimbursement. She has helped hundreds of solo practitioners and multi-specialty groups optimize their revenue cycles through expert coding education and audit defense. Her deep understanding of CPT guidelines and payer behavior allows her to translate complex regulations into practical, doctor-friendly strategies.



Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.

