Are you ready to grow up your business? Contact Us
Email Address: info@billingmedtech.com
Are you ready to grow up your business? Contact Us
You treat heel pain, diabetic ulcers, infections, fractures, and chronic foot conditions every day. But if your podiatry collection rates are low, your practice still struggles financially. Claims are denied. Patient balances remain unpaid. Documentation does not support CPT codes. Small billing gaps slowly drain revenue.
Most podiatrists assume collections improve simply by increasing patient volume. That is rarely true. In most U.S. podiatry practices, low collection rates come from documentation gaps, modifier misuse, Medicare routine foot care rules, and weak denial follow-up inside the revenue cycle.
The good news is this. These problems are predictable. And they are fixable with structured billing discipline.
This guide explains how podiatry collection rates work, why they drop, and how to improve them using real-world U.S. billing strategies.
Podiatry collection rates measure how much money your practice actually collects compared to what it should collect.
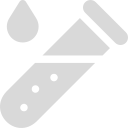
There are two main metrics.
Gross collection rate measures total payments divided by total charges billed.
Net collection rate measures payments collected divided by allowed amounts after contractual adjustments from payers.
The net collection rate is the more accurate performance indicator. For most healthy podiatry practices, the net rate should be 95 percent or higher. If your rate drops below 90 percent, there is usually a denial or follow-up problem inside your revenue cycle management process.
Podiatry is heavily affected by Medicare policies, Local Coverage Determinations, frequency limits, and modifier rules. These rules change often and are enforced strictly.
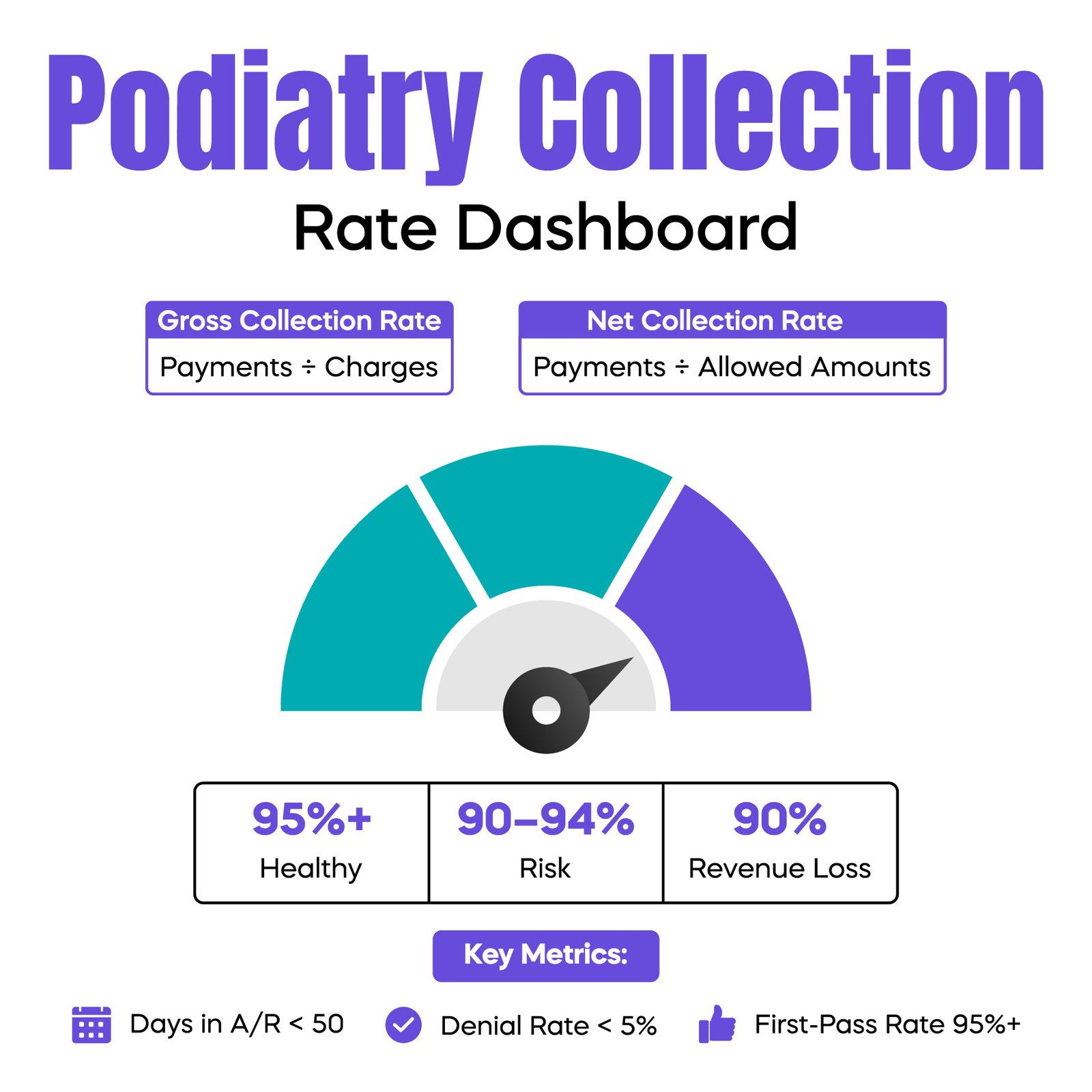
One common issue is routine foot care denial. Medicare does not cover routine foot care unless the patient has a qualifying systemic condition, such as diabetes with neuropathy or peripheral vascular disease. The documentation must clearly show the systemic diagnosis, class findings, and the date the patient was last seen for the systemic condition. If even one element is missing, the Medicare Administrative Contractor will deny the claim.
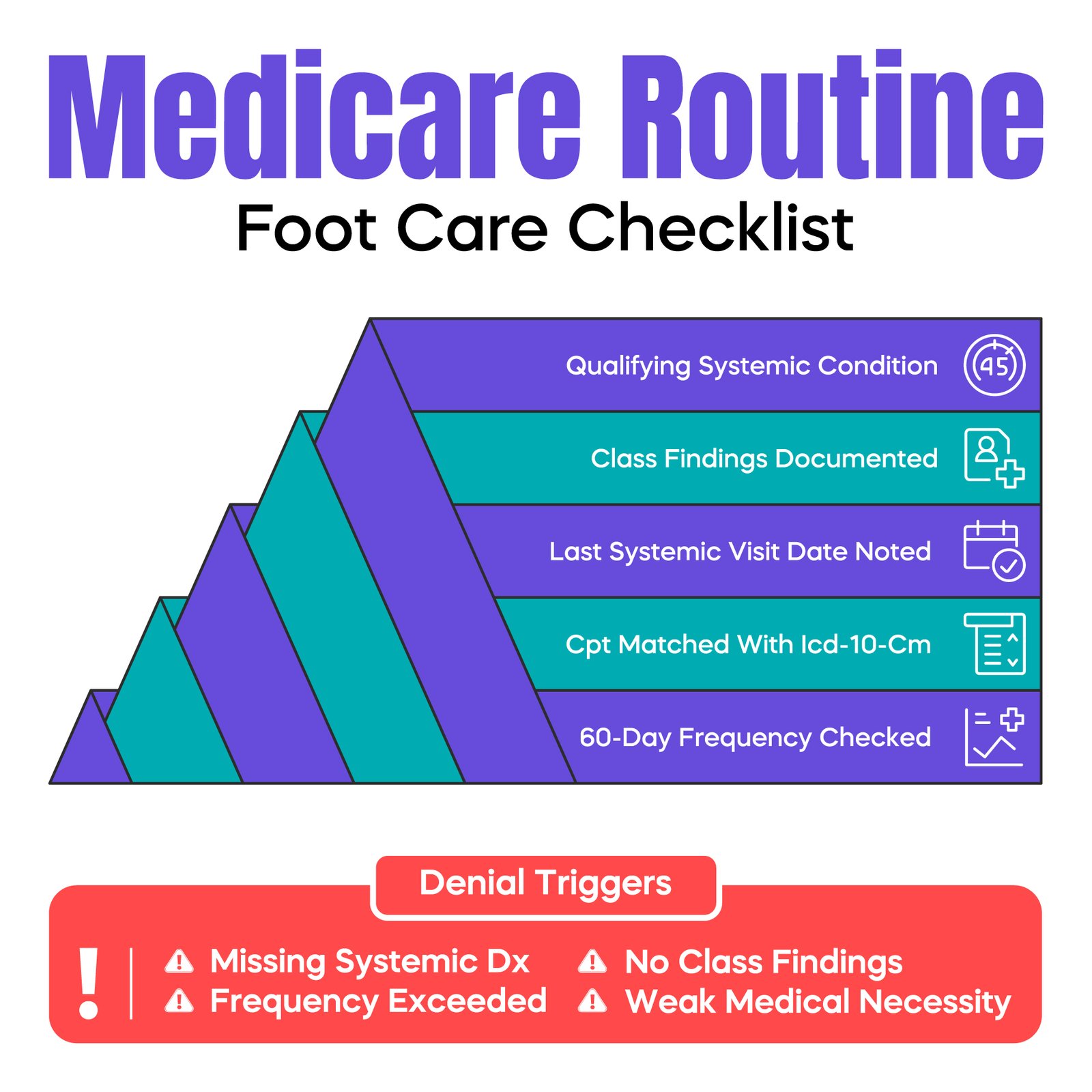
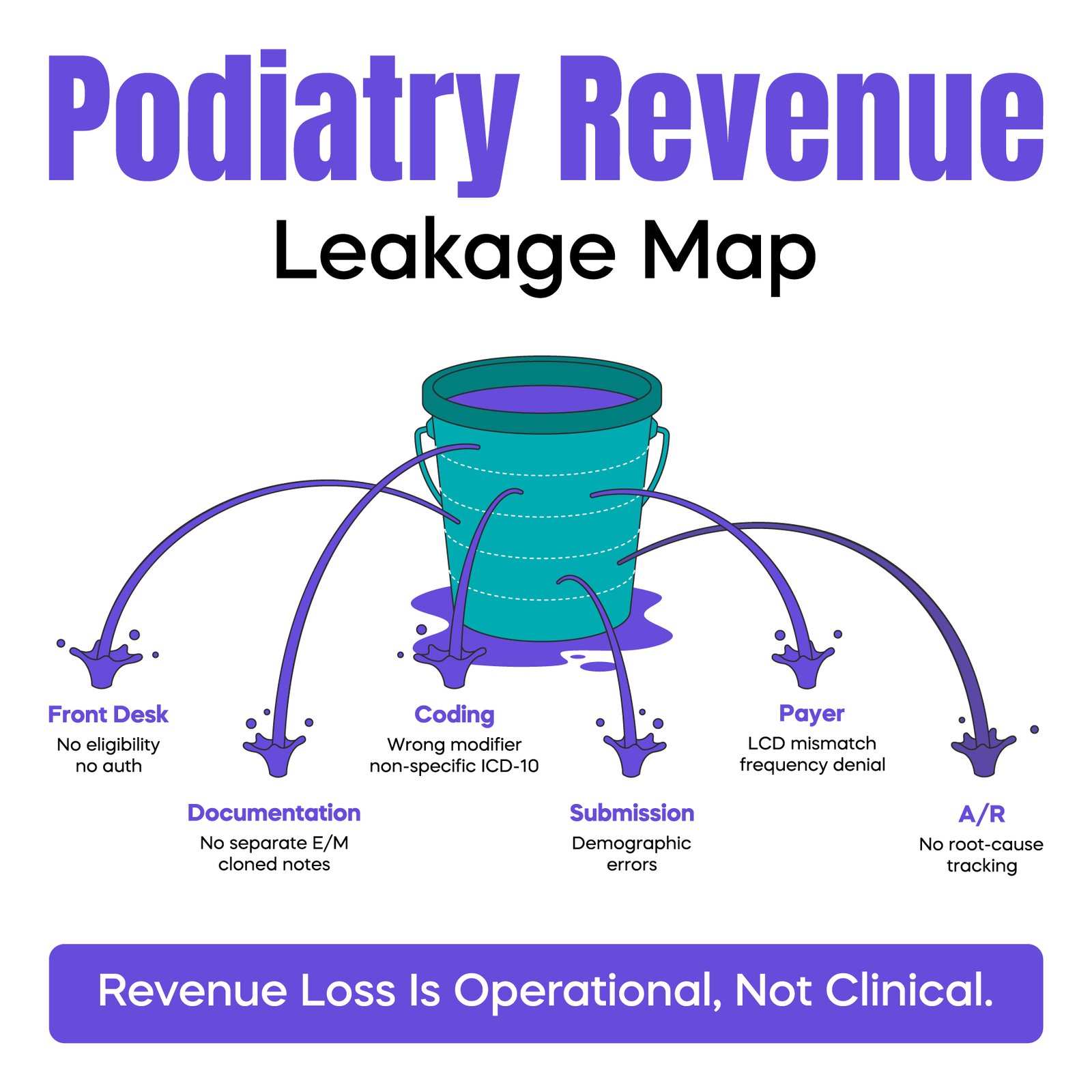
Modifier misuse is another major problem. Modifier 25 is often appended to evaluation and management codes when a procedure such as nail debridement is performed. However, if the documentation does not show a separate, medically necessary evaluation beyond the procedure, the payer may deny or downcode the E/M service. Overuse of Modifier 25 is also a common audit trigger.
Documentation misalignment between CPT and ICD-10-CM codes also reduces collection rates. For example, billing diabetic foot care without clearly documenting neuropathy or angiopathy leads to medical necessity denials. Clearinghouses may not catch this. But payer review systems often do.
High patient responsibility balances also reduce collections. Many podiatry procedures fall under deductibles or coinsurance. If benefits are not verified before the visit, patients are surprised by balances, and payment becomes delayed or uncollectible.
Finally, weak denial management keeps money locked in accounts receivable. Resubmitting a denied claim without correcting the root cause rarely works. Without structured tracking and follow-up, revenue quietly slips away.
Collection improvement starts at the front desk, not in billing.
Eligibility must be verified before every visit. Staff should confirm active coverage, deductible status, and whether routine foot care exclusions apply. Referral requirements and prior authorization rules must also be confirmed for surgical procedures or advanced wound care services.
When prior authorization is missed, most commercial payers issue automatic denials. These are often non-recoverable. Preventing the denial is easier than appealing it later.
Strong documentation protects revenue and reduces audit risk.
For Medicare routine foot care, documentation must clearly include the systemic condition, class findings, and medical necessity explanation. Notes should be specific. Generic or copied templates increase audit exposure.
When billing an E/M service with a procedure, the note must show a separately identifiable evaluation. This includes separate history, examination elements, and medical decision-making. Simply documenting the procedure does not justify billing both services.
Cloned documentation from EHR templates is frequently flagged during CMS audits. Internal chart reviews should be performed quarterly to confirm compliance.
Most podiatry revenue comes from a small number of CPT codes, including nail debridement, callus paring, common E/M levels, and minor surgical procedures.
Run monthly reports from your practice management system. Review denial rates by CPT code. Identify which codes trigger frequent payer rejections. Evaluate whether modifiers are used correctly and whether documentation supports medical necessity.
If one CPT code consistently shows a high denial percentage, analyze the cause. Often, a small documentation adjustment can significantly improve collections.
Local Coverage Determinations vary by region. What one Medicare Administrative Contractor allows may differ in another state.
Many podiatrists do not review LCD updates regularly. When documentation requirements change, practices may continue billing the old way without realizing the policy has shifted. This can lower collection rates for months before anyone notices the trend.
Assign responsibility within your practice to monitor MAC bulletins and CMS updates at least quarterly. Small regulatory changes often have a direct revenue impact.
Every denial should be investigated carefully. Identify the denial reason code. Review the documentation. Correct the error. Then resubmit or appeal with supporting records.
For example, if the denial code indicates a lack of medical necessity, simply resubmitting the claim without adding detailed documentation will not result in payment. Supporting clinical notes and correct ICD-10-CM coding must accompany the appeal.
Denial categories should be tracked monthly. If routine foot care denials increase, retraining providers on documentation requirements may resolve the issue quickly.
Improving patient collections significantly increases overall podiatry collection rates.
Copays should be collected before the visit. Deductible status should be discussed clearly. Providing cost estimates for non-covered services reduces disputes later.
Many successful podiatry practices use a credit card on file policy. This reduces aging balances and improves cash flow. Payment plans may be offered for larger surgical balances, but structured agreements should be documented.
Without measurement, improvement is impossible.
Track the net collection rate monthly. Monitor days in accounts receivable. Ideally, A/R should remain under 50 days. If it rises above 60 days, follow-up systems need attention.
First-pass claim acceptance rate should also be monitored. A low rate signals coding or eligibility issues. Denial rate by payer should be analyzed separately, since some commercial payers apply stricter foot care policies than Medicare.
First, Modifier 25 overuse can attract payer scrutiny. If your E/M volume appears unusually high compared to procedural volume, this may trigger review.
Second, diabetic foot care frequency limits are often ignored. Medicare generally limits routine foot care services to once every 60 days unless additional medical necessity is documented. Billing too frequently without justification leads to denials and possible recoupment.
Third, outdated ICD-10-CM coding can reduce medical necessity support. If the diagnosis does not reflect the most specific level available, reimbursement may be affected. Regular coding education is essential.
If your net collection rate remains below benchmark levels despite internal corrections, external review may be appropriate.
Signs include high denial rates, aging accounts receivable beyond 90 days, frequent staff turnover, and repeated payer audits.
Podiatry billing requires a detailed understanding of CMS policies, CPT modifiers, and LCD documentation standards. Specialized revenue cycle management support can sometimes identify structural problems internal teams overlook.
Arj Fatima is a U.S. medical billing specialist with deep experience in podiatry billing, Medicare compliance, CPT coding, ICD-10 documentation, and revenue cycle management. She has worked with solo podiatrists and multi-location specialty practices to reduce denials, improve net collection rates, and prepare for CMS audits. Her expertise includes routine foot care compliance, modifier accuracy, LCD monitoring, and structured denial management systems designed specifically for foot and ankle practices.
Ready to optimize your revenue cycle? Our team is here to help. Contact us for a free consultation and see how Billing MedTech can make a difference for your practice.

© Billing MedTech. All Rights Reserved
In today’s fast-paced digital era, where technology continuously reshapes the future of businesses, organizations need a trusted partner who can deliver innovation with reliability. That’s where Billing MedTech comes in.